Risk of erectile dysfunction associated with use of 5-α reductase inhibitors for benign prostatic hyperplasia or alopecia: population based studies using the Clinical Practice Research Datalink
BMJ 2016; 354 doi: https://doi.org/10.1136/bmj.i4823 (Published 22 September 2016) Cite this as: BMJ 2016;354:i4823
- Katrina Wilcox Hagberg, epidemiologist1,
- Hozefa A Divan, epidemiologist2,
- Rebecca Persson, research associate1,
- J Curtis Nickel, professor of urology3,
- Susan S Jick, professor of epidemiology and biostatistics1
- 1Boston Collaborative Drug Surveillance Program, Boston University School of Public Health, Lexington, MA 02421, USA
- 2New England Research Institute, Watertown, MA, USA
- 3Kingston General Hospital, Queen’s University, Kingston, Ontario, Canada
- Correspondence to: K W Hagberg khagberg{at}bu.edu
- Accepted 15 August 2016
Abstract
Objective To estimate the risk of erectile dysfunction in men who used 5-α reductase inhibitors to treat benign prostatic hyperplasia or alopecia.
Design Cohort studies with nested case-control analyses.
Setting UK Clinical Practice Research Datalink.
Population Two populations of men free of risk factors for erectile dysfunction and other sexual dysfunction or its treatment: men aged 40 or more with benign prostatic hyperplasia who received a prescription for a 5-α reductase inhibitor (finasteride or dutasteride) or α blocker, or both, and men aged 18-59 with alopecia.
Exposures In the benign prostatic hyperplasia study, exposures were classified as 5-α reductase inhibitors only, 5-α reductase inhibitors+α blockers, or α blockers only. In the alopecia study, exposures were finasteride 1 mg or no treatment.
Main outcome measures Cases were men with a diagnosis of erectile dysfunction or treatment (procedure or prescription for a phosphodiesterase type 5 inhibitor) during follow-up. We calculated incidence rates and adjusted incidence rate ratios with 95% confidence intervals. We also conducted nested case-control analyses to control for major confounders, and calculated adjusted odds ratios with 95% confidence intervals.
Results In the population with benign prostatic hyperplasia (n=71 849), the risk of erectile dysfunction was not increased with use of 5-α reductase inhibitors only (incidence rate ratio 0.92, 95% confidence interval 0.85 to 0.99; odds ratio 0.94, 95% confidence interval 0.85 to 1.03) or 5-α reductase inhibitors+α blocker (1.09, 0.99 to 1.21, 0.92; 0.80 to 1.06) compared with α blockers only, and remained null regardless of number of prescriptions or timing of use. The risk of erectile dysfunction increased with longer duration of benign prostatic hyperplasia, regardless of exposure. For the alopecia population (n=12 346), the risk of erectile dysfunction was not increased for users of finasteride 1 mg compared with unexposed men with alopecia (1.03, 0.73 to 1.44; 0.95, 0.64 to 1.41).
Conclusion 5-α reductase inhibitors do not seem to significantly increase the risk of incident erectile dysfunction, regardless of indication for use. Risk of erectile dysfunction increased with longer duration of benign prostatic hyperplasia.
Introduction
The 5-α reductase inhibitors finasteride (5 mg) and dutasteride (0.5 mg) are primarily used to treat benign prostatic hyperplasia, with a second indication for finasteride 1 mg to treat alopecia. Though benign prostatic hyperplasia itself is an independent risk factor for erectile dysfunction,1 evidence suggests that 5-α reductase inhibitors may independently increase the risk of adverse sexual side effects,2 3 4 5 6 7 8 9 10 potentially through induction of androgen deficiency by inhibition of 5-α reductase and reduction in available 5-α dihydrotestosterone.11 Further, these adverse effects may be persistent or irreversible even when treatment is discontinued.5 9 10 11 In addition, a recent meta-analysis of sexual adverse events from the few published clinical trials available evaluating the efficacy of finasteride 1 mg for alopecia reported that the data are limited, of poor quality, and insufficient for establishing the safety profile of the drug for alopecia treatment.12
Changes to the labeling of finasteride were announced by the Food and Drug Administration in 2011 and 2012 to include a list of reported sexual adverse events.13 Of particular concern is that many reports of sexual dysfunction were in previously healthy young men using finasteride 1 mg for alopecia.9 Increasing patient activism, including establishment of a research foundation for “post-finasteride syndrome,” is indicative of growing alarm and the need for awareness and research on long term complications of 5-α reductase inhibitor use.14 Finally, assessment of the safety of 5-α reductase inhibitors for benign prostatic hyperplasia and alopecia is warranted owing to the large sales volume15 and prescribing of these drugs for hair loss to otherwise healthy young men. We conducted two cohort studies with nested case-control analyses to evaluate the risk of erectile dysfunction in men who used 5-α reductase inhibitors to treat benign prostatic hyperplasia or alopecia. We also estimated the rate of non-erectile dysfunction sexual dysfunctions (ejaculatory disorder, psychosexual dysfunction, and low libido) in these populations of 5-α reductase inhibitor users.
Methods
Data source
This study was conducted using the UK Clinical Practice Research Datalink (CPRD), a large, longitudinal, population based electronic medical record database that contains data on approximately 10 million people. Participating general practitioners contribute data in an anonymous format, including medical diagnoses, lifestyle details (eg, smoking, body mass index), details of hospital stays and specialist visits, and deaths, as well as details of all drugs prescribed, including formulation and dosing instructions. Data in the CPRD are collected prospectively, and all information on diseases and prescriptions is recorded in the absence of a study hypothesis, so there is no risk of recall bias. Validation studies have indicated that the recorded data are of high accuracy, with more than 90% of information from the manual medical records present in the general practitioner’s office recorded on the computer.16 17
Patient populations
The study period was 1 January 1992 (the year that finasteride was first available in the UK) through 31 December 2011. We limited the end of the study period to 31 December 2011 owing to changes in the indication for use of phosphodiesterase type 5 inhibitors (drugs indicated for the treatment of erectile dysfunction, which were approved for the treatment of benign prostatic hyperplasia in 2012) and changes in the UK Quality and Outcomes Framework (which prompts all general practitioners to document whether they have asked all men with diabetes about potential erectile dysfunction).
We identified all men in the CPRD who had a prescription for either a 5-α reductase inhibitor (finasteride or dutasteride) or an α blocker (alfuzosin, doxadosin, indoramin, prazosin, tamsulosin, and terazosin), or both, plus a diagnosis of benign prostatic hyperplasia or prostatism recorded at any time prior to the first prescription date through three months after (to allow time for general practitioners to record diagnoses made by specialists). During the study period, α blockers were the only available alternative pharmaceutical treatment for benign prostatic hyperplasia, thus we chose them as an active comparator to ensure that all men included in the study population had benign prostatic hyperplasia severe enough to require treatment. α blockers are also indicated for hypertension; therefore to be included users were required to have a diagnosis of benign prostatic hyperplasia or prostatism. We defined the date of cohort entry as the date of the first prescription for a 5-α reductase inhibitor or α blocker in the patient’s record. The study population was restricted to men who were aged 40 years or older and who had at least three years of history before the cohort entry date. A three year requirement was selected to ensure that men were free from sexual dysfunction before cohort entry and were new users of a study drug. These men (n=71 849) comprised the population with benign prostatic hyperplasia (fig 1⇓).

Fig 1 Flowchart for population with benign prostatic hyperplasia
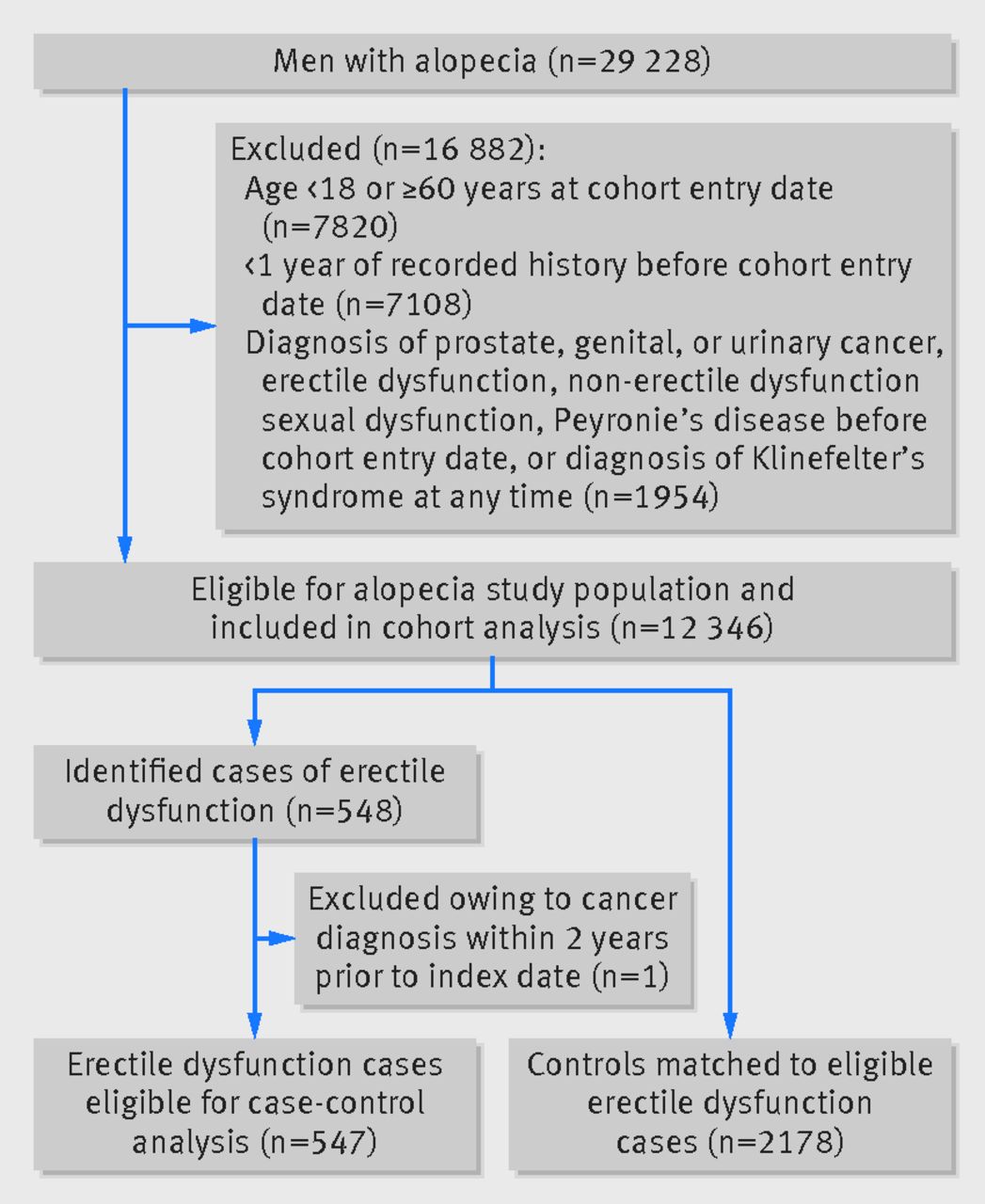
We then separately identified all men in the CPRD who had a diagnosis of alopecia (male pattern baldness) between 1 January 2002 (the first year finasteride was prescribed for alopecia) and 31 December 2011, were aged 18-59, and had at least one year of history in their record before cohort entry. We defined the date of cohort entry as 1 January 2002 (the start of the study period), the date of the first alopecia diagnosis occurring after 1 January 2002, or the date of the first prescription for finasteride 1 mg where the prescription was recorded before the alopecia diagnosis. We required only one year of history for this analysis because young men have shorter records in the CPRD, and because there is less concern that patients in this age group have a history of sexual dysfunction or finasteride prescriptions prior to cohort entry. These men (n=12 346) comprised the population with alopecia (fig 2⇓).

{kind=link}
{kind=link}
Men with prostate, genital, or urinary cancer, prostatectomy or orchidectomy, history of erectile dysfunction diagnosis or treatment (eg, procedures or drugs used to treat erectile dysfunction), other sexual dysfunctions (eg, ejaculatory disorder, psychosexual dysfunction, low libido), or Peyronie’s disease before cohort entry, or Klinefelter’s syndrome recorded at any time were excluded from both the benign prostatic hyperplasia and the alopecia study populations.
Exposure definition
Using the recorded prescribing details, we calculated the duration of each prescription for 5-α reductase inhibitors as the quantity of pills divided by the number of pills prescribed each day. For the benign prostatic hyperplasia population, person days of exposure were accrued in the following categories: 5-α reductase inhibitors only, 5-α reductase inhibitors plus α blockers, and α blockers only, as well as by timingof use, categorized as current (period of filled use plus 30 days), recent (days 31-90 after the end of current use), past (days 91-180 after the end of current use), and distant past use (the number of days after the end of past use). We considered men in the alopecia population to be unexposed until they received a prescription for finasteride 1 mg. Person days of finasteride 1 mg use were accrued and categorized as current (period of filled use plus 30 days), recent (days 31-90 after the end of current use), or past use (all days after the end of recent use). The censor date in both populations was the first of the following: end of record, death, or record of prostate, urinary, genital, pituitary, or adrenal cancers, prostatectomy, orchidectomy, end of study period (31 December 2011), date of being aged 60 years (for those in the alopecia population only), or date of being a case.
Case identification
Cases of erectile dysfunction were men with one or more of the following recorded during follow-up: diagnosis of erectile dysfunction or impotence, prescription for a phosphodiesterase type 5 inhibitor (eg, sildenafil, tadalafil, or vardenafil) where the strength and quantity prescribed was indicated for treatment of erectile dysfunction, or record of procedures for treatment of erectile dysfunction (eg, penile prosthesis, penile injection, or other operations for treatment of erectile dysfunction). We defined the erectile dysfunction index date—the date that the man was identified as a case—as the earliest date of diagnosis, date of prescription for a phosphodiesterase type 5 inhibitor, or date of procedure for erectile dysfunction.
We also identified men with a diagnosis of a non-erectile dysfunction sexual dysfunction (ejaculatory disorder, psychosexual dysfunction, or low libido) recorded during follow-up to assess the rate of these outcomes. In studies on the non-erectile dysfunction sexual dysfunction cohort, the index date was the date that the man was given a diagnosis of ejaculatory disorder, psychosexual dysfunction, or low libido, whichever came first.
Matching criteria for nested case-control analyses
Using the cases of erectile dysfunction identified in the cohort analyses, we conducted nested case-control analyses to control for age, calendar time, and risk factors for erectile dysfunction. We further excluded cases with a diagnosis of cancer (other than non-melanoma skin cancer) within two years before the index date because cancer and its treatment may be associated with the development of erectile dysfunction (n=46 in the population with benign prostatic hyperplasia, n=1 in the alopecia population). For each eligible case, we used risk set sampling to match up to four controls from the population on year of birth (within two years), general practice attended, index date (the same index date as the matched case), and year the patient started in the database (within two years). Controls were required to be present in the study population on the index date (that is, the index date had to fall between the candidate control’s cohort entry date and censor date) and must not have had a diagnosis of or treatment for erectile dysfunction before the index date, or have had a diagnosis of any cancer (other than non-melanoma skin cancer) within two years prior to the index date. For the benign prostatic hyperplasia case-control match, 5762 erectile dysfunction cases had four matched controls each, whereas one case was matched to three controls, three cases were matched to two controls, and one case was matched to one control. For the alopecia case-control match, 539 of the cases had four matched controls each, whereas four cases were matched to three controls and three cases were matched to two controls.
Covariates of interest
We assessed the presence of covariates of interest at the cohort entry date (cohort studies) and the index date (case-control analyses). Covariates of interest in this study included known or suspected risk factors for erectile dysfunction and non-erectile dysfunction sexual dysfunctions: age, calendar time, body mass index (<18.5, 18.5-24.9, 25-29.9, ≥30, unknown), smoking status (never, smoker, former smoker, unknown), non-erectile dysfunction sexual dysfunction (eg, ejaculatory disorders, psychosexual dysfunction, low libido), Peyronie’s disease, diabetes, hypertension, cardiovascular disease, atherosclerosis or coronary heart disease, kidney failure or dialysis, cancer, depression, alcohol misuse, and drug misuse. We also identified patients who received prescriptions for β blockers, which have been associated with erectile dysfunction, within six months prior to the cohort entry date and index date. We classified each patient in the benign prostatic hyperplasia population by whether they switched between study drugs (α blockers and 5-α reductase inhibitors) during follow-up. We also evaluated the duration of benign prostatic hyperplasia (<6 months, 6 months-1 year, 1-2 years, 2-5 years, ≥5 years).
Statistical analyses
For the benign prostatic hyperplasia cohort analysis, we calculated incidence rates of erectile dysfunction and incidence rate ratios with 95% confidence intervals for each exposure category, by age, calendar year, and timing of use (current, recent, past, or distant past). In the benign prostatic hyperplasia nested case-control analysis, we used conditional logistic regression to calculate crude odds ratios and 95% confidence intervals, as well as odds ratios adjusted for body mass index, smoking status, non-erectile dysfunction sexual dysfunctions, Peyronie’s disease, hypertension, diabetes, hyperlipidemia, depression, orchitis, alcohol misuse, switching status, and duration of benign prostatic hyperplasia, to estimate the risk of erectile dysfunction in users of 5-α reductase inhibitors only and 5-α reductase inhibitors+α blockers compared with use of α blockers only. Odds ratios approximate the incidence rate ratio through the use of risk set sampling.
For the alopecia cohort analysis, we calculated incidence rates of erectile dysfunction and incidence rate ratios with 95% confidence intervals for unexposed men and for users of finasteride 1 mg, by age, calendar year, and timing of finasteride 1 mg use (current, recent, and past). In the alopecia nested case-control analysis, we used conditional logistic regression to calculated crude odds ratios and 95% confidence intervals, as well as odds ratios adjusted for body mass index, smoking status, duration of benign prostatic hyperplasia, non-erectile dysfunction sexual dysfunctions, hypertension, diabetes, hyperlipidemia, cardiovascular disease, liver disease, depression, alcohol misuse, drug misuse, and receipt of a β blocker prescription within six months prior to the index date, to estimate the risk of erectile dysfunction in users of finasteride 1 mg for alopecia compared with unexposed men with alopecia. In both the benign prostatic hyperplasia and the alopecia nested case-control analyses, we stratified the case-control results by age group to assess effect modification. We also assessed the potential for misclassification of cases with erectile dysfunction in sensitivity analyses restricted to the cases with codes that supported the erectile dysfunction diagnosis, including the presence of multiple erectile dysfunction diagnoses or prescriptions for phosphodiesterase type 5 inhibitors, surgical procedures, or referrals to specialty care, and their matched controls. Finally, we calculated incidence rates of non-erectile dysfunction sexual dysfunctions and incidence rate ratios with 95% confidence intervals for both the benign prostatic hyperplasia population and the alopecia population. We did not conduct a nested case-control study for those outcomes owing to the low number of non-erectile dysfunction sexual dysfunction cases identified. All statistical analyses for this study were conducted using SAS statistical software version 9.3 (SAS Institute, Cary, NC).
Patient involvement
No patients were involved in setting the research question or the outcome measures, nor were they involved in developing plans for design or implementation of the study. No patients were asked to advise on interpretation or writing of results. There are no plans to disseminate the results of the research to study participants or the relevant patient community.
Results
Erectile dysfunction in the benign prostatic hyperplasia population
Overall, 71 849 men with benign prostatic hyperplasia were eligible for inclusion; at cohort entry, 8977 received a prescription for 5-α reductase inhibitors only, 2592 for 5-α reductase inhibitors+α blockers, and 60 280 for α blockers only (table 1⇓). At cohort entry, users of 5-α reductase inhibitors only and 5-α reductase inhibitors+α blockers were older and more likely to switch between study drugs during follow-up compared with users of α blockers only. Users of 5-α reductase inhibitors+α blockers had more comorbidities compared with users of 5-α reductase inhibitors only and α blockers only.
Characteristics of benign prostatic hyperplasia population. Values are numbers (percentages) unless stated otherwise
We identified 5814 cases of erectile dysfunction, of whom 5022 (86.4%) had a diagnosis of erectile dysfunction or impotence and 792 (13.6%) were identified based on prescriptions for a phosphodiesterase type 5 inhibitor. The incidence rate of erectile dysfunction was lowest among users of 5-α reductase inhibitors only (15.3 per 1000 person years, 95% confidence interval 14.3 to 16.5), and similar among users of 5-α reductase inhibitors+α blockers (19.2 per 1000 person years, 17.4 to 21.1) and α blockers only (20.1 per 1000 person years, 19.6 to 20.7). Compared with users of α blockers only, the adjusted incidence rate ratios for users of 5-α reductase inhibitors only and 5-α reductase inhibitors+α blockers were 0.92 (95% confidence interval 0.85 to 0.99) and 1.09 (0.99 to 1.21), respectively (table 2⇓).
Incidence rates (IR) and incidence rate ratios (IRR) for erectile dysfunction by exposure in cohort with benign prostatic hyperplasia
In the nested case-control analysis, cases of erectile dysfunction were more likely than matched controls to be overweight or obese (as measured by body mass index) or to have a diagnosis of non-erectile dysfunction sexual dysfunction, hypertension, diabetes, hyperlipidemia, depression, orchitis, or alcohol misuse before the index date. Cases also had longer duration of benign prostatic hyperplasia compared with controls and were more likely to switch between study drugs at some time before the index date (table 3⇓). There was no effect on the risk of erectile dysfunction from use of 5-α reductase inhibitors only (adjusted odds ratio 0.94, 95% confidence interval 0.85 to 1.03) or 5-α reductase inhibitors+α blockers (0.92, 0.80 to 1.06) compared with α blockers only (table 4⇓). The results remained null regardless of number of prescriptions received or timing of use. To assess effect modification we stratified the estimates by switching status and duration of benign prostatic hyperplasia. The risk of erectile dysfunction was higher for switchers than for non-switchers, independent of exposure. Risk of erectile dysfunction also increased with longer duration of benign prostatic hyperplasia, independent of exposure (table 4⇓). Compared with users of α blockers only with duration of benign prostatic hyperplasia of less than six months, the risk of erectile dysfunction for men with a duration of six months to one year was 1.15 (95% confidence interval 1.01 to 1.32) for users of α blockers only and 1.20 (0.93 to 1.56) for users of 5-α reductase inhibitors only, which increased to 2.80 (2.50 to 3.13) and 2.54 (2.13 to 3.03) for users of α blockers only and 5-α reductase inhibitors only, respectively, with duration of benign prostatic hyperplasia for five or more years. The pattern was similar for users of 5-α reductase inhibitors+α blockers. Finally, we assessed effect modification by diabetes status by stratifying on the presence or absence of diabetes before the index date. The reference in this analysis was users of α blockers only with no diabetes. The increase in risk of erectile dysfunction was present among men with diabetes, whereas the risk was null for men without diabetes, regardless of exposure to α blockers only, 5-α reductase inhibitors only, or 5-α reductase inhibitors+α blockers (table 4⇓).
Nested case-control analysis: characteristics of cases with erectile dysfunction and controls in benign prostatic hyperplasia population. Values are numbers (percentages) unless stated otherwise
Nested case-control analysis: risk of erectile dysfunction by exposure in benign prostatic hyperplasia population
When we stratified by age to evaluate effect modification, the risk of erectile dysfunction was similar to that of the main analysis, regardless of age group. Among cases and controls aged 40-69 years, the adjusted odds ratio was 0.94 (95% confidence interval 0.82 to 1.06) for users of 5-α reductase inhibitors only and 0.96 (0.80 to 1.16) for users of 5-α reductase inhibitors+α blockers, whereas among cases and controls aged 70 years or older, the adjusted odds ratio was 0.89 (0.77 to 1.05) for users of 5-α reductase inhibitors only and 0.82 (0.65 to 1.03) for users of 5-α reductase inhibitors+α blockers. The results were also not materially different from the main analysis when we conducted the sensitivity analysis restricted to the erectile dysfunction cases who had additional codes that supported the erectile dysfunction diagnosis (n=4960, 86%) and their matched controls (adjusted odds ratio 0.89 (95% confidence interval 0.80 to 1.00) for 5-α reductase inhibitors only and 0.85 (0.73 to 1.00) for 5-α reductase inhibitors+α blockers, compared with α blockers only).
Erectile dysfunction in the alopecia population
We identified 12 346 men with alopecia who were eligible for inclusion in the alopecia population, of whom 463 received a prescription for finasteride 1 mg at cohort entry (n=868 of the alopecia population who used finasteride 1 mg at some time during follow-up) and 11 883 were unexposed at cohort entry (table 5⇓). At cohort entry, users of finasteride 1 mg for alopecia were younger and more likely to have depression or to have received a prescription for β blockers within the prior six months, whereas unexposed men with alopecia had more diagnoses of lower urinary tract symptoms. We identified 547 cases of erectile dysfunction, of whom 491 (89.8%) had a diagnosis of erectile dysfunction or impotence and 56 (10.2%) were identified based on prescriptions for a phosphodiesterase type 5 inhibitor. The incidence rates of erectile dysfunction were similar for users of finasteride 1 mg (10.1 per 1000 person years (95% confidence interval 7.0 to 13.9) and unexposed men (9.8 per 1000 person years, 8.9 to 10.7) (table 6⇓). The incidence rate ratio, adjusted for age and calendar time, was 1.13 (95% confidence interval 0.80 to 1.58) for users of finasteride 1 mg compared with unexposed men with alopecia (table 6⇓).
Characteristics of population with alopecia. Values are numbers (percentages) unless stated otherwise
Incidence rates (IRs) and incidence rate ratios (IRRs) for erectile dysfunction by exposure in analysis of alopecia cohort
In the nested case-control analysis, cases of erectile dysfunction were more likely than matched controls to be overweight or obese, be former smokers, or have non-erectile dysfunction sexual dysfunction, hypertension, diabetes, hyperlipidemia, cardiovascular disease, liver disease, depression, and alcohol and drug misuse before the index date (table 7⇓). The adjusted odds ratio for erectile dysfunction was 0.94 (95% confidence interval 0.64 to 1.40) for users of finasteride 1 mg compared with unexposed men (table 8⇓). The risk of erectile dysfunction increased with increasing number of finasteride 1 mg prescriptions, from 0.69 (95% confidence interval 0.33 to 1.40) for one prescription to 1.43 (0.71 to 2.90) for 10 or more prescriptions, but none of the odds ratios were statistically significant. The risk of erectile dysfunction was null, regardless of timing of use or time since the last prescription (table 8⇓). When we stratified by age to evaluate effect modification, the risk of erectile dysfunction in users of finasteride 1 mg was higher in men aged 40-59 years (adjusted odds ratio 1.45, 95% confidence interval 0.87 to 2.44) than in men aged 18-39 years (0.50, 0.26 to 0.98), although the difference in risk by age was not statistically significant.
Nested case-control analysis: characteristics of cases with erectile dysfunction and controls in alopecia population. Values are numbers (percentages) unless stated otherwise
Nested case-control analysis: risk of erectile dysfunction by exposure in alopecia population. Values are numbers (percentages) unless stated otherwise
Since men with alopecia who were prescribed finasteride 1 mg were generally healthier and had fewer risk factors for erectile dysfunction than men with alopecia not taking finasteride 1 mg, we conducted additional analyses to determine whether the null results could be explained by differences in the baseline health status of the two groups. We first restricted the analysis to cases and controls who did not have risk factors for erectile dysfunction (benign prostatic hyperplasia, non-erectile dysfunction sexual dysfunction, Peyronie’s disease, or orchitis) before the index date. The results were similar to those of the main analysis (adjusted odds ratio 0.97, 95% confidence interval 0.62 to 1.47). We also conducted an analysis restricted to “healthy” cases and controls (those with no diagnoses of hypertension, diabetes, hyperlipidemia, cardiovascular disease, liver disease, or cancer prior to the index date) and found no material differences in the results (0.74, 0.47 to 1.19).
When we conducted a sensitivity analysis restricted to cases of erectile dysfunction who had clinical codes that supported the erectile dysfunction diagnosis (n=332, 61%) and their matched controls, the odds ratio for users of finasteride 1 mg compared with unexposed men were null (adjusted odds ratio 1.49, 95% confidence interval 0.91 to 2.42). When the analysis was further restricted to the “healthy” cases and controls, the odds ratio was similar (0.74, 0.47 to 1.19).
Non-erectile dysfunction sexual dysfunctions
In the benign prostatic hyperplasia population, we identified 232 men with a non-erectile dysfunction sexual dysfunction diagnosis before the censor date (n=27 ejaculatory dysfunction, n=88 psychosexual dysfunction, n=115 low libido, and n=2 with multiple diagnoses recorded on the same date). The rate of non-erectile dysfunction sexual dysfunctions was 0.9 per 1000 person years (95% confidence interval 0.6 to 1.2) for users of 5-α reductase inhibitors only, 0.8 per 1000 person years (0.5 to 1.2) for users of 5-α reductase inhibitors+α blockers, and 0.8 per 1000 person years (0.6 to 0.9) for users of α blockers only. Compared with users of α blockers only, the incidence rate ratio of non-erectile dysfunction sexual dysfunction adjusted for age, calendar time, and timing of exposure was 1.35 (95% confidence interval 0.95 to 1.91) for users of 5-α reductase inhibitors only and 1.62 (0.79 to 2.72) for users of 5-α reductase inhibitors+α blockers. The rates were low and not significantly different by exposure when we considered ejaculatory dysfunction, psychosexual dysfunction, and low libido separately. For ejaculatory dysfunction, the incidence rate was 0.06 per 1000 person years (95% confidence interval 0.01 to 0.17) for users of 5-α reductase inhibitors only, 0.05 per 1000 person years (0.002 to 0.2) for 5-α reductase inhibitors+α blockers, and 0.10 per 1000 person years (0.06 to 0.14) for α blockers only. For psychosexual dysfunction, the incidence rate was 0.3 per 1000 person years (0.2 to 0.5) for users of 5-α reductase inhibitors only, 0.2 per 1000 person years (0.1 to 0.4) for 5-α reductase inhibitors+α blockers, and 0.3 per 1000 person years (0.0 to 0.4) for α blockers only. For low libido, the incidence rate was 0.5 per 1000 person years (0.3 to 0.7) for users of 5-α reductase inhibitors only, 0.65 per 1000 person years (0.3 to 0.9) for 5-α reductase inhibitors+α blockers, and 0.4 per 1000 person years (0.3 to 0.4) for α blockers only.
In the alopecia population, we identified 104 men with a diagnosis of non-erectile dysfunction sexual dysfunction before the censor date (n=40 ejaculatory dysfunction, n=16 psychosexual dysfunction, n=46 low libido, and n=1 with multiple diagnoses recorded on the same date). The rate of non-erectile dysfunction sexual dysfunctions for users of finasteride 1 mg was 2.79 per 1000 person years (95% confidence interval 1.42 to 4.98) and 1.80 per 1000 person years (1.46 to 2.19) for unexposed men with alopecia. The incidence rate ratio of non-erectile dysfunction sexual dysfunction adjusted for age, calendar time, and timing of use was 1.55 (95% confidence interval 0.98 to 2.47) for users of finasteride 1 mg compared with unexposed men with alopecia. The rates were low and not significantly different by exposure when we considered ejaculatory disorder, psychosexual dysfunction, and low libido separately. For ejaculatory disorder, the incidence rate was 0.3 per 1000 person years (0.0 to 1.4) for users of finasteride 1 mg and 0.8 per 1000 person years (0.5 to 1.0) for unexposed men. For psychosexual dysfunction, the incidence rate was 0.0 per 1000 person years (0.0 to 0.2) for users of finasteride 1 mg and 0.3 per 1000 person years (0.2 to 0.5) for unexposed men. For low libido, the incidence rate was 0.8 per 1000 person years (0.2 to 2.3) for users of finasteride 1 mg and 0.8 per 1000 person years (0.6 to 1.1) for unexposed men.
Discussion
Overall, the results of our study suggest that 5-α reductase inhibitors do not increase the risk of incident erectile dysfunction, regardless of indication for use (benign prostatic hyperplasia or alopecia). In a population of men age 40 years and older with treated benign prostatic hyperplasia, there was no increase in risk of incident erectile dysfunction with use of 5-α reductase inhibitors (finasteride or dutasteride), alone or in combination with α blockers, compared with use of α blockers only. In addition, among men aged 18-59 with alopecia, there was no material increase in the risk of incident erectile dysfunction in men prescribed finasteride 1 mg compared with unexposed men with alopecia. Finally, the rates of non-erectile dysfunction sexual dysfunctions were low regardless of indication for 5-α reductase inhibitor use. The risk of erectile dysfunction increased with longer duration of benign prostatic hyperplasia, independent of exposure. This finding is noteworthy because UK prescribing guidelines during much of the study period recommended that α blockers be first line treatment for benign prostatic hyperplasia followed by a switch to, or addition of, 5-α reductase inhibitors when treatment with α blockers was not effective or when benign prostatic hyperplasia had progressed. Therefore, users of 5-α reductase inhibitors were likely to have benign prostatic hyperplasia for a longer duration, resulting in a higher risk for erectile dysfunction. The absence of increased risk of erectile dysfunction in users of 5-α reductase inhibitors with benign prostatic hyperplasia, as well as in users with alopecia, provides strong evidence against the hypothesis that 5-α reductase inhibitors independently increase the risk of erectile dysfunction.
Comparison with other studies
Results from clinical trials evaluating the efficacy of 5-α reductase inhibitors for the treatment of benign prostatic hyperplasia or prevention of prostate cancer suggest that these drugs increase the risk of erectile dysfunction, whereas our results were null. The relative risk of erectile dysfunction with use of 5-α reductase inhibitors in clinical trials for prevention of prostate cancer varied from 1.10 to 1.5,2 3compared with placebo, and the changes in sexual function associated with 5-α reductase inhibitors were typically noted within the first year of treatment, and became comparable with placebo by study termination. Evidence from clinical trials evaluating the efficacy of finasteride only, α blockers only, and combination treatment for benign prostatic hyperplasia have also suggested that use of 5-α reductase inhibitors, alone or in combination with α blockers, increases the risk of erectile dysfunction compared with placebo. The risks based on published results range from 0.8 to 1.5 for finasteride only compared with α blockers only, whereas the risks of combination treatment range from 1.4 to 1.8 compared with α blockers only.18 19 20 21 Our results yielded no differences in the risk of erectile dysfunction by type of 5-α reductase inhibitor (finasteride or dutasteride), which is consistent with results of a clinical trial that compared the efficacy and safety of finasteride with dutasteride.22 A post-marketing surveillance study (n=14 772) conducted in the UK in 1992-94, shortly after finasteride was first marketed, found that impotence/ejaculation was reported in 2.1% of patients prescribed finasteride, similar to the rate of erectile dysfunction in our benign prostatic hyperplasia study population.23
The results of published studies evaluating the efficacy of finasteride 1 mg to treat alopecia have been inconsistent,6 7 8 9 24 25 26 27 whereas our results were null. An increase of sexual side effects has been reported in clinical trials evaluating the efficacy of finasteride 1 mg for treatment of alopecia, with approximately 4% of men treated with finasteride reporting sexual side effects compared with approximately 2% of men treated with placebo.6 7 8 9 A systematic review of six clinical trials that reported on the safety of finasteride 1 mg or 5 mg for treatment of alopecia compared with placebo, found an increased risk of patient reported erectile dysfunction (relative risk 2.22, 95% confidence interval 1.03 to 4.78).24 In contrast, three small trials conducted in clinical settings with short term follow-up reported no significant difference in erectile dysfunction adverse events.25 26 27
The clinical trials evaluating 5-α reductase inhibitors for the treatment of benign prostatic hyperplasia and alopecia have also identified non-erectile dysfunction sexual dysfunctions as adverse effects of 5-α reductase inhibitor use. A systematic review of available randomized clinical trials reported that ejaculatory dysfunction was more common among users of 5-α reductase inhibitors for treatment of benign prostatic hyperplasia compared with users of placebo (odds ratio 2.73, P<0.001) in trials comparing α blockers and 5-α reductase inhibitors, whereas in trials comparing 5-α reductase inhibitors with α blockers the prevalence of ejaculatory dysfunction was similar for users of both drugs (odds ratio 0.7, P=0.42).28 Another review of data from clinical trials found that low libido was reported as an adverse event for 2-5% of patients treated with 5-α reductase inhibitors compared with 1-3% of the placebo group.10 A small cross sectional study of men attending an outpatient clinic for sexual dysfunction (n=48 patients using 5-α reductase inhibitors) reported a higher prevalence of low libido among users of 5-α reductase inhibitors compared with men who did not use 5-α reductase inhibitors; however, there were no significant differences in the prevalence of premature ejaculation or ejaculatory volume.29 In comparison, in our study there was no evidence of a substantial increase in risk of non-erectile dysfunction sexual dysfunctions, and the rates were less than three events per 1000 person years regardless of indication for use, lower than those reported in clinical trials. In the UK Clinical Practice Research Datalink (CPRD), codes used to identify non-erectile dysfunction outcomes (ejaculatory disorder, psychosexual dysfunction, and low libido) are neither specific nor used regularly, consistently, or correctly (because of the close relation with diagnosis of erectile dysfunction) by general practitioners. Thus it is likely that we missed cases of non-erectile dysfunction sexual dysfunctions, and therefore the rates reported here are underestimates. Our results for non-erectile dysfunction sexual dysfunctions should be interpreted cautiously in light of the data limitations for these outcomes as well as the small number of exposed cases of non-erectile dysfunction sexual dysfunction identified (n=58 exposed non-erectile dysfunction cases in the benign prostatic hyperplasia population and n=10 exposed non-erectile dysfunction cases in the alopecia population).
Unlike the published clinical trials, men in both our benign prostatic hyperplasia study population and our alopecia study population were free from diagnoses of and treatments for erectile dysfunction prior to cohort entry. In addition, patients with a history of other strong risk factors for erectile dysfunction prior to cohort entry, such as prostate, genital, or urinary cancer, or a history of prostatectomy or orchiectomy, were excluded from the study population or censored on subsequent diagnosis of these major erectile dysfunction and non-erectile dysfunction sexual dysfunction risk factors after cohort entry. Importantly, to be identified as a case of erectile dysfunction in our study men were required either to have a diagnosis or to have received treatment (pharmaceutical or procedural) for erectile dysfunction recorded by the general practitioner in their electronic medical record before the censoring date, whereas all of the clinical trials used questionnaires completed by participants to assess changes in sexual function. Thus, a major strength of our study is that it captured clinically meaningful erectile dysfunction diagnoses that came to the general practitioner’s attention. In our study, users of 5-α reductase inhibitors, particularly in combination with α blockers, were generally less healthy than users of α blockers only. Men with benign prostatic hyperplasia who have multiple medical problems may have less sex or may less often bring up concerns about sexual function to their doctor, whereas the doctors may be more concerned with treating the other conditions than about the sexual health of their patients; that is, users of 5-α reductase inhibitors may be less likely to have their erectile dysfunction diagnosed (detection bias). If this were the case, then the true incidence of erectile dysfunction among users of 5-α reductase inhibitors alone or in combination might be higher than we detected in our study.
Alopecia and prostate enlargement/benign prostatic hyperplasia are both related to the conversion of testosterone to dihydrotestosterone, which is stimulated by increased activity of the enzyme 5-α reductase.10 Owing to underlying biochemistry, men who have benign prostatic hyperplasia or alopecia may be at an increased risk of erectile dysfunction compared with men without either condition, regardless of treatment. Our study was designed to control for confounding by indication. In the benign prostatic hyperplasia study, we used an active comparator (α blockers only) rather than non-exposed, to control for confounding by severity and duration of benign prostatic hyperplasia, whereas men in our alopecia study population were required to have a recorded diagnosis of alopecia. The number of patients in our benign prostatic hyperplasia study population identified as a case of erectile dysfunction (8%) was similar to the proportion of patients who self reported having erectile dysfunction in clinical trials (0% to 16%),2 3 19 20 21 whereas the rates of erectile dysfunction among men with alopecia in our study were similar to those reported among men in general.30 31 Also, erectile dysfunction has not been reported as a common side effect of the α blockers evaluated in our study.32 Approximately 46% of the patients who used α blockers only in our benign prostatic hyperplasia population were prescribed tamsulosin, followed by alfuzosin (12%) and doxazosin (11%); in our study, the risk of erectile dysfunction did not differ by type of α blocker prescribed (data not shown). We do not believe that the null results found in our study were due to use of comparison groups who had an increased baseline risk for erectile dysfunction.
Strengths and limitations of this study
Strengths of our population based study included the use of CPRD, a large, validated, longitudinal primary care database known for high accuracy of diagnoses and completeness of drug prescribing data. We found known risk factors to be independently associated with risk for erectile dysfunction (eg, increased body mass index, hypertension, hyperlipidemia, diabetes), providing confidence in the quality of the data and its ability to detect associations between benign prostatic hyperplasia treatments and risk of erectile dysfunction. As all information on diseases and drug exposures is recorded in the absence of a study hypothesis, there is no risk of recall bias. The mean length of follow-up was greater than four years. We further controlled our analyses for a range of potential confounders, including non-erectile dysfunction sexual dysfunction, hypertension, diabetes, body mass index, smoking status, depression, and duration of benign prostatic hyperplasia. By excluding men who had insufficient history in their medical record before cohort entry we reduced the risk of including men who had used the study drugs before cohort entry, as well as reduced the risk of including men with prevalent, rather than incident, erectile dysfunction.
A major strength of our study is that it relied on doctor recorded diagnoses, rather than patient reported changes in sexual function, to identify cases. Finally, the population of men prescribed 5-α reductase inhibitors and α blockers for benign prostatic hyperplasia (n=71 849) and the population of men with alopecia (n=12 346, of which 868 received prescriptions for finasteride 1 mg during follow-up) described in our study are robust and are the largest populations of “real world” users of these drugs evaluated to date. This allowed us to study the effects of these drugs as prescribed in routine clinical practice. This is not possible in clinical trials given their smaller size and highly selected study populations.
There are some limitations to consider. Drug information in the CPRD covers written, not dispensed prescriptions; therefore we cannot be sure that patients used all prescribed drugs. However, the relative risks did not change among those with repeat (≥2) prescriptions, suggesting that this did not affect the results. During our study period, phosphodiesterase type 5 inhibitors were available in the UK for prescriptions through private sources; therefore, we may have missed some cases of erectile dysfunction where these drugs were prescribed outside of the general practitioner’s office. This is unlikely to be differential by exposure category, and thus may have biased the true estimates toward the null. Objective measures of the severity of benign prostatic hyperplasia are not captured in the CPRD data, thus we were unable to assess the impact of severity on the results. We were able to identify codes relating to lower urinary tract symptoms; however, these codes are symptom based, are not specific to benign prostatic hyperplasia, and might be related to other urological and medical conditions. Severe lower urinary tract symptoms are known to be associated with erectile dysfunction, but in our study such symptoms did not confound the relation between exposure and outcome in either the benign prostatic hyperplasia population or the alopecia population. Although the populations of men evaluated in these studies were robust, in some of the analyses the numbers of exposed cases were small, particularly for non-erectile dysfunction sexual dysfunctions (n=36 exposed erectile dysfunction cases in the alopecia population, n=58 exposed non-erectile dysfunction sexual dysfunction cases in the benign prostatic hyperplasia population, and n=10 exposed in the alopecia population); thus the results for these analyses should be interpreted with caution. However, it is important to note that the CPRD is one of the few observational data sources in the world where these numbers of erectile dysfunction and non-erectile dysfunction sexual dysfunction cases could be identified and evaluated. Our study results suggest that the duration of benign prostatic hyperplasia is a strong independent risk factor for erectile dysfunction; therefore, studies evaluating the incidence of erectile dysfunction after use of 5-α reductase inhibitors or α blockers should be interpreted cautiously and with consideration to the duration of benign prostatic hyperplasia.
Conclusions and policy implications
The results of our study provide evidence that 5-α reductase inhibitors do not increase the risk of clinically meaningful incident erectile dysfunction in men who are free of sexual dysfunction and major risk factors (eg, prostate, genital, or urinary cancers, surgical procedures), regardless of indication for use (benign prostatic hyperplasia or alopecia). The risk of erectile dysfunction increases with longer duration of benign prostatic hyperplasia, which should be accounted for in the design of future studies evaluating the safety of 5-α reductase inhibitors. Since benign prostatic hyperplasia and alopecia are common conditions in men and 5-α reductase inhibitors are primary drug treatments for these conditions, the results of this study provide reassurance that these drugs are not associated with a materially important increased risk of clinically meaningful erectile dysfunction in every day clinical practice.
What is already known on this topic
Erectile dysfunction and other sexual dysfunctions have been reported as adverse effects of 5-α reductase inhibitors in clinical trial settings
Benign prostatic hyperplasia, one of the indications for use of 5-α reductase inhibitors, is a risk factor for erectile dysfunction and other sexual dysfunctions
What this study adds
Our study results provide evidence that 5-α reductase inhibitors do not increase the risk of clinically meaningful incident erectile dysfunction or non-erectile dysfunction sexual dysfunction in men who are free of sexual dysfunction and major risk factors (eg, prostate, genital, or urinary cancers, surgical procedures), regardless of indication for use (benign prostatic hyperplasia or alopecia)
The risk of erectile dysfunction increased with longer duration of benign prostatic hyperplasia independent of exposure which should be accounted for in the design of future studies evaluating the safety of 5-α reductase inhibitors
Footnotes
Contributors: KWH participated in the study conception and design, identified the study population and reviewed the cases, cleaned the data and conducted the statistical analysis, participated in the interpretation of results, and drafted and revised the paper. She is a guarantor. HAD participated in the interpretation of the results and revised the paper. RP participated in identification of the study population and cases, cleaned the data and conducted the statistical analysis, participated in the interpretation of results, and revised the paper. JCN participated in the study conception, interpretation of the results, and revised the paper. SSJ participated in the study conception and design, interpretation of the results, and revised the paper. She is a guarantor. All authors had access to the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. All authors reviewed and approved the final version of the paper for publication.
Funding: This study was funded by a grant (5R21DK100820-02) from the United States National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases. All authors had independence from the funding source.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that: all authors have support from an United States National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases grant (5R21DK100820-02) for the submitted work; KWH, HAD, RP, and SSJ have no relationships that might have an interest in the submitted work in the previous three years; JCN had a financial relationship with GlaxoSmithKline three years ago consulting on a non-related patent lawsuit and has a current non-financial relationship with GlaxoSmithKline for access to REDUCE trial data for research outside of the submitted work; their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and none of the authors have non-financial interests that may be relevant to the submitted work.
Ethical approval: The protocols for this study were reviewed and approved by the independent scientific advisory committee of the CPRD (protocol Nos 15_132R and 15_223R).
Data sharing: No additional data available.
Transparency: The guarantors (KWH and SSJ) affirm that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/.