
Heart Rate Variability and Sympathetic Activity Is Modulated by Very Low-Calorie Ketogenic Diet

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects Recruitment
2.2. The Two Diet Programs
2.3. Stages of the Study
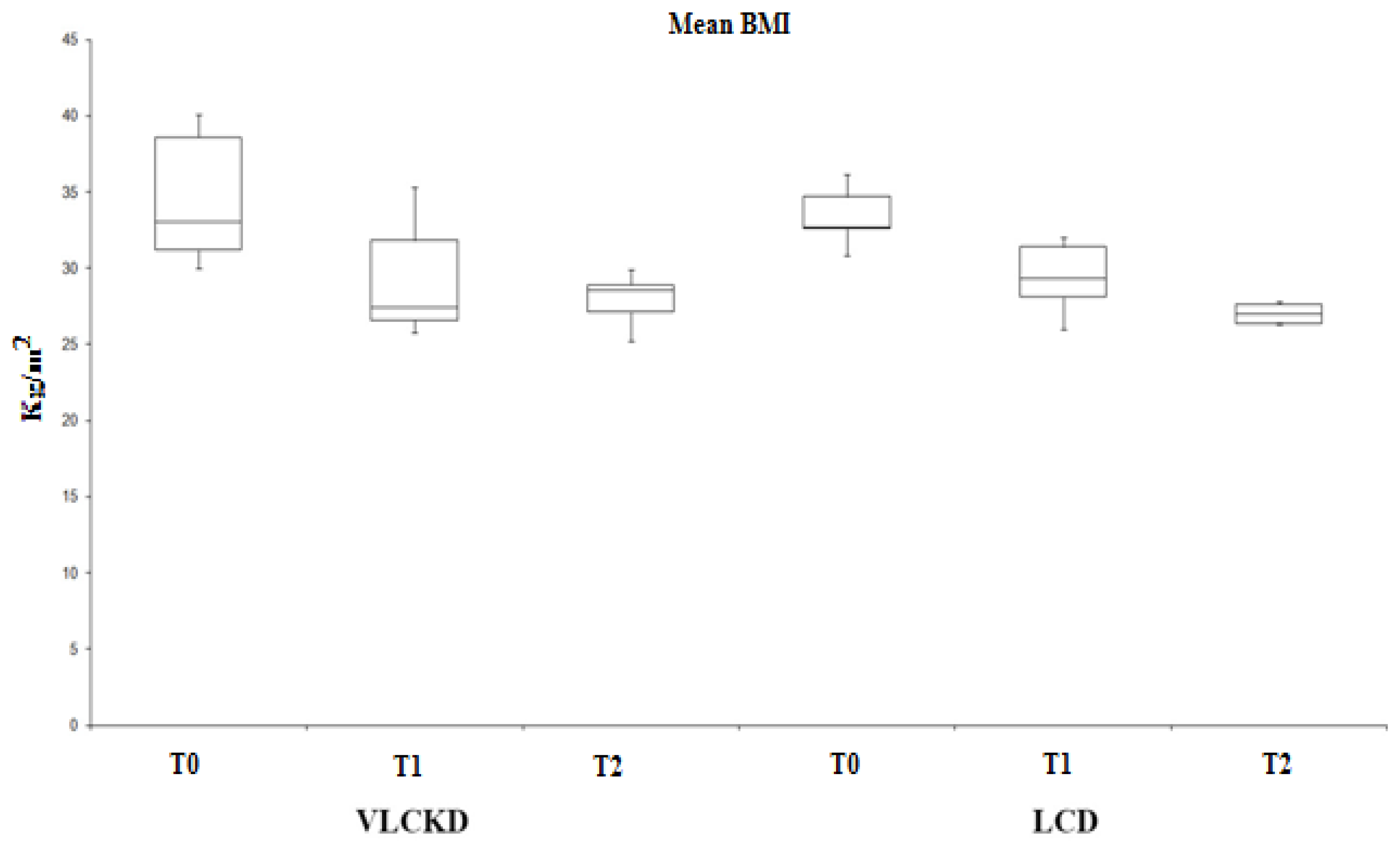
- Time T0: initial phase in which the subjects are recruited and assigned to one or the other group. The subjects undergo a general medical examination and dietary evaluation by completing the food diary; instrumental evaluation of anthropometric parameters: BMI by weight measurement (b ilancia SECA, Tecnomed s.a.s., Verona, Italy, maximum capacity 150 Kg and approximation not exceeding 100 g) and height (SECA 711 stadiometer, Tecnomed s.a.s., Verona, Italy), body circumferences, skin folds; blood chemistry profile; analysis of the oxidation state by evaluating the plasma dosage of free radicals and endogenous antioxidant agents; electrocardiographic recording (ECG) and measurement of heart rate variability (HRV).
- T1 time: period necessary to achieve weight loss by administering the appropriate diet. During this phase, subjects must reach 80% of the expected weight loss goal and, on a weekly basis, instrumental body composition checks are carried out by means of BIA, instrumental evaluation of anthropometric parameters and, only for the VLCKD group, verification of the permanence of the subjects in the condition of dietary ketosis is carried out by monitoring the plasma levels of β-hydroxybutyrate. At the end of this phase, the subjects of both groups are subjected to the repetition of the whole series of blood chemistry and instrumental tests proposed in phase 1.
- Time T2: subjects belonging to both groups continue to follow the hypocaloric dietary regimen assigned to them until the predetermined weight loss is achieved. Even at the end of this phase, the subjects are subjected to the repetition of the battery of blood chemistry and instrumental tests carried out in the first two phases. Furthermore, in this last phase, all subjects are prescribed an aerobic exercise program at 60–70% of maximum heart rate, lasting 60–90 min and twice a week.
2.4. Heart Rate Variability (HRV)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiessl, G.R.R.; Laessle, R.G. Stress inhibits PYY secretion in obese and normal weight women. Eat. Weight Disord.-Stud. Anorexia Bulim. Obes. 2016, 21, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Berntson, G.G.; Bigger, J.T.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Berthoud, H.R.; Morrison, C. The brain, appetite, and obesity. Annu. Rev. Psychol. 2008, 59, 55–92. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Benelli, M.; Brancaleoni, M.; Dainelli, G.; Merlini, D.; Negri, R. Middle and Long-Term Impact of a Very Low-Carbohydrate Ketogenic Diet on Cardiometabolic Factors: A Multi-Center, Cross-Sectional, Clinical Study. High Blood Press. Cardiovasc. Prev. 2015, 22, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Dahlin, M.; Elfving, A.; Ungerstedt, U.; Amark, P. The ketogenic diet influences the levels of excitatory and inhibitory amino acids in the CSF in children with refractory epilepsy. Epilepsy Res. 2005, 64, 115–125. [Google Scholar] [CrossRef]
- Douris, N.; Desai, B.N.; Fisher, F.M.; Cisu, T.; Fowler, A.J.; Zarebidaki, E.; Nguyen, N.L.T.; Morgan, D.A.; Bartness, T.J.; Rahmouni, K.; et al. Beta-adrenergic receptors are critical for weight loss but not for other metabolic adaptations to the consumption of a ketogenic diet in male mice. Mol. Metab. 2017, 6, 854–862. [Google Scholar] [CrossRef]
- Draghici, A.E.; Taylor, J.A. The physiological basis and measurement of heart rate variability in humans. J. Physiol. Anthropol. 2016, 35, 22. [Google Scholar] [CrossRef] [Green Version]
- Evangeliou, A.; Vlachonikolis, I.; Mihailidou, H.; Spilioti, M.; Skarpalezou, A.; Makaronas, N.; Prokopiou, A.; Christodoulou, P.; Liapi-Adamidou, G.; Helidonis, E.; et al. Application of a ketogenic diet in children with autistic behavior: Pilot study. J. Child Neurol. 2013, 18, 113–118. [Google Scholar] [CrossRef]
- Thio, L.L. Hypothalamic hormones and metabolism. Epilepsy Res. 2012, 100, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Triggiani, A.I.; Valenzano, A.; Ciliberti, M.A.; Moscatelli, F.; Villani, S.; Monda, M.; Messina, G.; Federici, A.; Babiloni, C.; Cibelli, G. Heart rate variability is reduced in underweight and overweight healthy adult women. Clin. Physiol. Funct. Imaging 2017, 37, 162–167. [Google Scholar] [CrossRef]
- Orban, G.; Bombardi, C.; Marino Gammazza, A.; Colangeli, R.; Pierucci, M.; Pomara, C.; Pessia, M.; Bucchieri, F.; Arcangelo, B.; Smolders, I.; et al. Role(s) of the 5-HT2C Receptor in the Development of Maximal Dentate Activation in the Hippocampus of Anesthetized Rats. CNS Neurosci. Ther. 2014, 20, 651–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrowski, K.; Wintermann, G.B.; Joraschky, P.; Päßler, S. Chewing after stress: Psychosocial stress influences chewing fre-quency, chewing efficacy, and appetite. Psychoneuroendocrinology 2014, 48, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Schiavone, S.; Neri, M.; Trabace, L.; Turillazzi, E. The NADPH oxidase NOX2 mediates loss of parvalbumin interneurons in traumatic brain injury: Human autoptic immunohistochemical evidence. Sci. Rep. 2017, 7, 8752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turillazzi, E.; Baroldi, G.; Silver, M.D.; Parolini, M.; Pomara, C.; Fineschi, V. A systematic study of a myocardial lesion: Colliquative myocytolysis. Int. J. Cardiol. 2005, 104, 152–157. [Google Scholar] [CrossRef]
- Appelhans, B.M.; Pagoto, S.L.; Peters, E.N.; Spring, B.J. HPA axis response to stress predicts short-term snack intake in obese women. Appetite 2010, 54, 217–220. [Google Scholar] [CrossRef] [Green Version]
- Boison, D. New insights into the mechanisms of the ketogenic diet. Curr. Opin. Neurol. 2017, 30, 187–192. [Google Scholar] [CrossRef] [Green Version]
- Adam-Perrot, A.; Clifton, P.; Brouns, F. Low-carbohydrate diets: Nutritional and physiological aspects. Obes. Rev. 2006, 7, 49–58. [Google Scholar] [CrossRef]
- Valenzano, A.; Polito, R.; Trimigno, V.; Di Palma, A.; Moscatelli, F.; Corso, G.; Sessa, F.; Salerno, M.; Montana, A.; Di Nunno, N.; et al. Effects of very low calorie ketogenic diet on the orexinergic system, visceral adipose tissue, and ROS production. Antioxidants 2019, 8, 643. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Polito, R.; Lovino, A.; Finaldi, A.; Valenzano, A.; Nigro, E.; Corso, G.; Sessa, F.; Asmundo, A.; Di Nunno, N.; et al. Short-term physiological effects of a very low-calorie ketogenic diet: Effects on adiponectin levels and inflammatory states. Int. J. Mol. Sci. 2020, 21, 3228. [Google Scholar] [CrossRef]
- Messina, A.; Bitetti, I.; Precenzano, F.; Iacono, D.; Messina, G.; Roccella, M.; Parisi, L.; Salerno, M.; Valenzano, A.; Maltese, A.; et al. Non-rapid eye movement sleep parasomnias and migraine: A role of orexinergic projections. Front. Neurol. 2018, 9, 95. [Google Scholar] [CrossRef] [Green Version]
- Precenzano, F.; Ruberto, M.; Parisi, L.; Salerno, M.; Maltese, A.; Vagliano, C.; Messina, G.; Di Folco, A.; Di Filippo, T.; Roccella, M. Executive functioning in preschool children affected by autismspectrum dis-order: A pilot study. Acta Med. 2017, 33, 35. [Google Scholar]
- Viggiano, E.; Monda, V.; Messina, A.; Moscatelli, F.; Valenzano, A.; Tafuri, D.; Cibelli, G.; De Luca, B.; Messina, G.; Monda, M. Cortical spreading depression produces a neuroprotective effect activating mitochondrial uncoupling protein-5. Neuropsychiatr. Dis. Treat. 2016, 12, 1705–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monda, M.; Viggiano, A.; Mondola, R.; Viggiano, E.; Messina, G.; Tafuri, D.; De Luca, V. Olanzapine blocks the sympathetic and hyperthermic reactions due to cerebral injection of orexin A. Peptides 2008, 29, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, A.; Nicodemo, U.; Viggiano, E.; Messina, G.; Viggiano, A.; Monda, M.; De Luca, B. Mastication overload causes an increase in O2- production into the subnucleus oralis of the spinal trigeminal nucleus. Neuroscience 2010, 166, 416–421. [Google Scholar] [CrossRef]
- Viggiano, A.; Vicidomini, C.; Monda, M.; Carleo, D.; Carleo, R.; Messina, G.; Viggiano, A.; Viggiano, E.; De Luca, B. Fast and low-cost analysis of heart rate variability reveals vegetative alterations in noncomplicated diabetic patients. J. Diabetes Its Complicat. 2009, 23, 119–123. [Google Scholar] [CrossRef]
- Esposito, M.; Serpe, F.P.; Diletti, G.; Messina, G.; Scortichini, G.; La Rocca, C.; Baldi, L.; Amorena, M.; Monda, M. Serum levels of polychlorinated dibenzo-p-dioxins, polychlorinated dibenzofurans and polychlorinated biphenyls in a population living in the Naples area, southern Italy. Chemosphere 2014, 94, 62–69. [Google Scholar] [CrossRef]
- Sessa, F.; Messina, G.; Russo, R.; Salerno, M.; Castruccio Castracani, C.; Distefano, A.; Li Volti, G.; Calogero, A.E.; Cannarella, R.; Mongioi’, L.M.; et al. Consequences on aging process and human wellness of generation of nitrogen and oxygen species during strenuous exercise. Aging Male 2020, 23, 14–22. [Google Scholar] [CrossRef]
- Tirabassi, G.; Boscaro, M.; Arnaldi, G. Harmful effects of functional hypercortisolism: A working hypothesis. Endocrine 2014, 46, 370–386. [Google Scholar] [CrossRef]
- Bertozzi, G.; Salerno, M.; Pomara, C.; Sessa, F. Neuropsychiatric and Behavioral Involvement in AAS Abusers. A Literature Review. Medicina 2019, 55, 396. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Salerno, M.; Fiorenzo, M.; Villano, I.; Viggiano, A.; Sessa, F.; Triggiani, A.I.; Cibelli, G.; Valenzano, A.; Marsala, G.; et al. Role of Sex Hormones in the Control of Vegetative and Metabolic Functions of Middle-Aged Women. Front. Physiol. 2017, 8, 773. [Google Scholar] [CrossRef] [Green Version]
- Monda, V.; Salerno, M.; Sessa, F.; Bernardini, R.; Valenzano, A.; Marsala, G.; Zammit, C.; Avola, R.; Carotenuto, M.; Messina, G.; et al. Functional Changes of Orexinergic Reaction to Psychoactive Substances. Mol. Neurobiol. 2018, 55, 6362–6368. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VLCKD OBESE SUBJECTS | LCD OBESE SUBJECTS | ||||||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | p-Value | |
| Participants | 7/6 | 7/6 | |||||
| (M/F) | |||||||
| Age | 48 ± 3 | 47 ± 3 | ns | ||||
| Height (m) | 1.67 ± 5 | 1.67 ± 3 | ns | ||||
| Weight (kg) | 91.33 ± 11 | 78.73 ± 9 | 77.8 ± 5 | 86.33 ± 7 | 79.3 ± 8.7 | 76.28 ± 9 | <0.001 |
| BMI (kg/m2) | 34.48 ± 5 | 27.7 ± 4 | 27.25 ± 6 | 33.4 ± 8 | 28.6 ± 4.5 | 26.85 ± 4 | <0.001 |
| Blood Ketones (MMOL/L) | 1.9 ± 0.05 | 0.6 ± 0.2 | 0 | 0 | 0 | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polito, R.; Valenzano, A.; Monda, V.; Cibelli, G.; Monda, M.; Messina, G.; Villano, I.; Messina, A. Heart Rate Variability and Sympathetic Activity Is Modulated by Very Low-Calorie Ketogenic Diet. Int. J. Environ. Res. Public Health 2022, 19, 2253. https://doi.org/10.3390/ijerph19042253
Polito R, Valenzano A, Monda V, Cibelli G, Monda M, Messina G, Villano I, Messina A. Heart Rate Variability and Sympathetic Activity Is Modulated by Very Low-Calorie Ketogenic Diet. International Journal of Environmental Research and Public Health. 2022; 19(4):2253. https://doi.org/10.3390/ijerph19042253
Chicago/Turabian StylePolito, Rita, Anna Valenzano, Vincenzo Monda, Giuseppe Cibelli, Marcellino Monda, Giovanni Messina, Ines Villano, and Antonietta Messina. 2022. "Heart Rate Variability and Sympathetic Activity Is Modulated by Very Low-Calorie Ketogenic Diet" International Journal of Environmental Research and Public Health 19, no. 4: 2253. https://doi.org/10.3390/ijerph19042253