FAQs on Protecting Yourself from COVID-19 Aerosol Transmission
Shortcut to this page: https://tinyurl.com/FAQ-aerosols
Version: 1.88, 13-Aug-2021
Click here to jump over the scientific & historical details and go straight to the recommendations,
Click here for automatic translation into many languages (choose your language from the menu)
0.1. What is the goal of these FAQs?
0.2. Who has written these FAQs?
0.3. I found a mistake, or would like something to be added or clarified, can you do that?
0.4. Are these FAQs available in other languages?
0.5. Can I use the information here in other publications etc.?
1. General questions about COVID-19 transmission
1.2. What is the relative importance of the routes of transmission?
1.5 Are all infected people equally contagious?
1.7. Where can I find more scientific information at a higher level about aerosol transmission?
2. General questions about aerosol transmission
2.1. What is aerosol transmission?
2.2 What is the size of infectious aerosols?
2.3 What factors control how many infectious aerosols are exhaled?
2.4. Where do aerosols of different sizes deposit in the human respiratory tract?
2.7. How long does the SARS-CoV-2 remain infectious in aerosols?
2.8. Does temperature affect the survival of the virus in the air?
2.9. Does relative humidity (RH) affect transmission?
2.8. Is there an analogy for aerosol transmission?
2.9. Does that mean that smoking can help spread the virus?
2.10. Can pollution aerosols help spread the virus?
3. Protecting ourselves from aerosol transmission
3.1. At what distance from an infected person can I get infected?
3.2. Do the 1-2 m or 6 feet guidelines guarantee lack of infection indoors?
3.3. How long does one need to inhale infectious aerosol to be infected?
3.4. How long can the virus stay in the air indoors?
3.5. How can I protect myself from aerosol transmission indoors?
3.6. Is there a way to remember all the things I need to reduce or avoid?
3.7 Aren’t your recommendations the same as Japan’s 3 Cs?
3.8 Is there a way to understand the relative risk of different environments?
3.9 Is there a more quantitative way to investigate ways to reduce aerosol transmission?
4.1 Is there a risk of aerosol transmission outdoors?
4.2. Does UV light from the sun kill the virus?
4.3. Can I catch COVID-19 just by passing by someone indoors or outdoors?
4.4. Is it safe to eat outdoors at a restaurant?
4.5. Is it safe to go to the swimming pool, beach, or park?
5. Risk for specific situations
5.1. Is it safe to take a taxi cab or rideshare?
5.2. Is it safe to travel by airplane?
5.4 What do you suggest for dental offices?
5.7. My specific situation is not here, what can I do?
6.1. Are singing or playing wind instruments indoors dangerous?
6.2. What kinds of instruments generate the most aerosol?
6.3. What are the current recommendations to reduce aerosol emissions for musicians?
6.4. What about playing music outdoors or using tents?
6.5. What research is ongoing about transmission for choirs and wind instruments?
6.6. What do you think of the masks being sold for singers?
7. Masks and other protections
7.1. Do masks work to reduce the aerosol spread of COVID-19?
7.2. What is the best type of mask?
7.3. How effective are different types of masks for the wearer and for others?
7.4. Do I need to wear a mask outside?
7.5. Is it OK to just wear the mask over my mouth and leave my nose out?
7.6. Is the fit of a mask important?
7.7. Where should I stand around someone with a poorly fitting mask?
7.8. Is it ok to remove my mask to talk?
7.10. Are transparent masks safe?
7.11. Is there an easy way to assess my mask at home?
7.12. Do I need eye protection?
7.13. Are face shields and masks interchangeable?
7.14. Are plexiglass barriers helpful?
8.1. What do you mean by ventilation?
8.2. Are windows a good way to increase ventilation?
8.3. How are public buildings ventilated?
8.4. How can we quantify the ventilation rate in a space?
9. Monitoring ventilation using CO2 levels
9.1. Can we use the CO2 level in a space to estimate whether ventilation is good or bad?
9.2. What are the limitations and caveats of the relationship between CO2 and infection risk?
9.4. What type of CO2 analyzers can be trusted?
9.5. Where should I put the CO2 meter in a large room?
9.6. Do you recommend measuring and displaying CO2 in all public places?
9.7. Can we instead measure the respiratory aerosols directly?
10. Filtering, and “air cleaning”
10.1. What filters should I use in my heating and/or air conditioning system?
10.2. Are portable air cleaners useful? Which types do you recommend?
10.3. What are HEPA portable air cleaners?
10.4. But if the virus is 0.1 μm, do HEPA / MERV filters (or masks) remove it from the air?
10.5. Is there a cheaper alternative to a HEPA air cleaner?
10.6. How do I select the right HEPA air cleaner? (or fan-filter cleaner)
10.7. Where should I place a HEPA air cleaner in a room?
10.8. How and when should filters be replaced?
10.10. Do you recommend portable air cleaners that are not based on filtration?
10.11. Do you recommend spraying disinfectants into indoor air to kill the virus?
10.12. Should we use humidifiers or dehumidifiers?
10.13. Should we keep indoor spaces hotter or colder to reduce transmission?
0. Questions about these FAQs
0.1. What is the goal of these FAQs?
The goal of these FAQs is to provide information to the general public in an efficient manner about how to prevent aerosol transmission of COVID-19, with the hope that this will allow more informed decision making by individuals or organizations. All of this information has been posted in Twitter and other forums, but can be difficult to find. Having multiple experts working together, and having the ability to update this information also improves its quality. These FAQs represent our best understanding at this time, and should always be similar or more stringent than information provided by CDC, WHO, and most regional & local health authorities. If your authority has a more stringent guideline than discussed here, follow that more stringent guideline.
0.2. Who has written these FAQs?
Scientists and engineers with many years of collective research experience related to indoor air quality, aerosol science, aerosol disease transmission, and engineered control systems for aerosols. Our contributors are active researchers investigating aerosol transmission of COVID-19 (see e.g. 1, 2, 3, and 4). Five of us were speakers at the recent Workshop on Airborne Transmission of COVID-19, organized by the US National Academies of Sciences, Engineering, and Medicine (the highest level scientific organization in the US). Three of us are members of a COVID-19 WHO expert group. Specifically, the writers of these FAQs include Professors :
- Prof. Linsey Marr (Virginia Tech, Fellow ISIAQ, AAAR, AGU, NAE)
- Prof. Shelly Miller (CU Boulder, Fellow ISIAQ)
- Prof. Kimberly Prather (UC San Diego, Fellow AAAS & AGU, NAE & NAS, CAICE Director)
- Prof. Charles Haas (Drexel University, Fellow NAE, AAM & SRA)
- Prof. William Bahnfleth (Penn State, Fellow ASHRAE, ASME & ISIAQ, Chair of ASHRAE Epidemic Task Force)
- Prof. Richard Corsi (Portland State, President ISIAQ Fellows)
- Prof. Julian Tang (Univ. of Leicester & UK National Health Svce, Clinical/Academic Virologist/Physician, Fellow RCP-Virology)
- Prof. Hartmut Herrmann (Dept. Head, Leibniz-Institute for Tropospheric Research (TROPOS), University of Leipzig; Head Joint Working Party ‘PM’ of GDCh, KRDL and ProcessNet).
- Prof. Krystal Pollitt (School of Public Health, Yale University, Chair of Health-Effects Working Group AAAR)
- Prof. Javier Ballester (Engineering School, Universidad de Zaragoza, and LIFTEC - Joint Centre Univ. Zaragoza/CSIC)
- Prof. Jose-Luis Jimenez (CU Boulder, Highly Cited Researcher (h-index = 124), Fellow AAAR & AGU).
Several additional scientists are also working with us to contribute to this document. If other experts are interested in contributing to these FAQs or other related efforts, please contact Jose.
We think that unfortunately WHO and CDC are being too slow to accept aerosol transmission, hence the need for these FAQs directly from the scientists.
0.3. I found a mistake, or would like something to be added or clarified, can you do that?
We will update these FAQs in response to feedback, to fix any mistakes, or to expand them in response to questions (as time allows). Please complete the form at this link with any updates, errors, suggestions etc. Please do not send questions via email or Twitter, as it is too cumbersome to try to keep track of those.
0.4. Are these FAQs available in other languages?
At present we are making or planning a lot of updates, in response to a lot of questions and requests. But Google can translate it into many languages automatically. See
- Traduccion al espanol
- Traduction au français
- German translation
- For other languages, go to this page and change the language at the top
0.5. Can I use the information here in other publications etc.?
You are welcome to use any of this as you see fit. There is no need to contact us for permission. We only ask that you give the link http://tinyurl.com/faqs-aerosol as the source of the information. Please include the date and version number given at the top, if possible. If you need an author list, just list the people above.
1. General questions about COVID-19 transmission
1.1. How can I get COVID-19?
There are 3 ways:
1. The “aerosol” path. Aerosols are also particles of saliva or respiratory fluid, but they are smaller than about 100 μm. For this reason they can linger more in the air, from tens of seconds to hours, and the smaller ones can travel long distances. They infect by being inhaled through the nose or mouth, or (less likely) by deposition on the eyes. They reach different parts of the human respiratory tract depending on their size. These are the green, yellow, and red dots in the figure below.
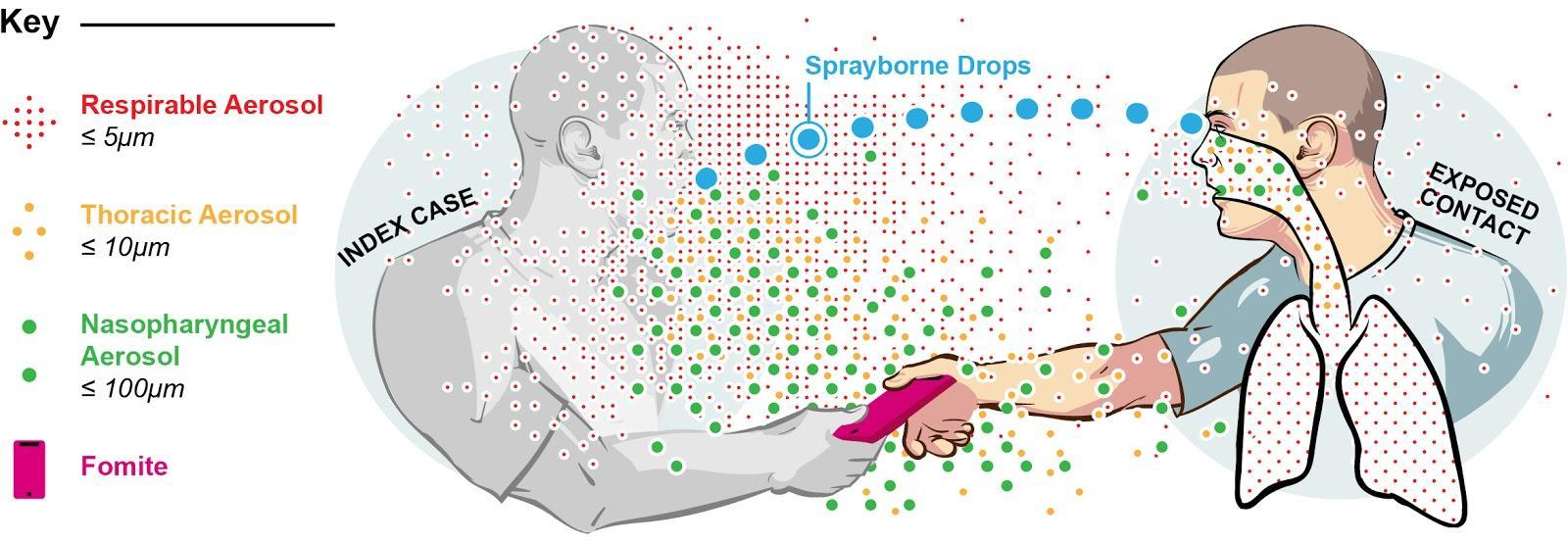
Figure: schematic representation of the droplet (blue) and aerosol (green, yellow, and red) infection pathways for a respiratory disease. Both travel through the air from the infected person to the susceptible person, but ballistic droplets infect by impact, and aerosols infect by inhalation. From Milton (2020), modified by the author (pers. comm.).
2. The “large droplet” or “ballistic droplet” path. Droplets are particles of saliva or respiratory fluid (larger than about 100 μm, with 1 μm = a millionth of a meter) that are expelled from infected individuals when coughing, sneezing, and to a lesser extent, talking. They fly ballistically (like a projectile) through the air, as in the famous “angry birds” video game. They infect by impacting on the mouth, nostrils, or eyes. They are the light blue ballistic droplets in the figure above. If they don’t hit someone, they fall to the ground in 1-2 m (3-6 ft).
3. The “fomite” path, through touching a surface that is contaminated with the SARS-CoV-2 virus, such as a light switch, a door handle, or someone else’s hand. That can transfer the virus onto your hand, and then you can infect yourself by touching your mouth, nostrils, or eyes.
1.2. What is the relative importance of the routes of transmission?
The relative importance will vary with people’s behavior, whether they wear masks and how well fit, whether they go indoors a lot or a little, whether they wash their hands often or not, etc. It will also vary with the setting.
In terms of general importance:
- The CDC’s Scientific Brief on transmission of SARS-CoV-2 lists inhalation of very fine droplets and aerosols first among the possible routes of transmission. Many scientists, including the authors of these FAQs, think that the aerosol pathway is the dominant route of transmission, with some contribution from fomites and ballistic droplets (from coughing and sneezing). This is based on a review of the available evidence, e.g. as summarized in this document and the table below. In particular for this virus there is a lot of transmission by people without (or very few) symptoms. Those people do not (or rarely) cough, so the usual “ballistic droplet” pathway is very diminished. People are also hyper aware of cough, and it does not seem credible that the pandemic spread is dominated by people coughing and scoring “direct hits” on other people’s eyes/nostrils/mouth. Many people don’t know how they were infected, and it is unlikely that they wouldn't remember a direct hit by a cough.
- Transmission by ballistic droplets and fomites are possible but thought to be less important.
- For the first year of the pandemic, CDC and WHO promoted large ballistic droplets and contamination of surfaces by them (i.e., fomites) as the main routes of transmission, while downplaying the importance of inhalation of aerosols. The reasons for the resistance of CDC and WHO to aerosol transmission and their adherence to ballistic droplet transmission despite lack of evidence are rooted in history, including errors in assumptions about traditional transmission routes.
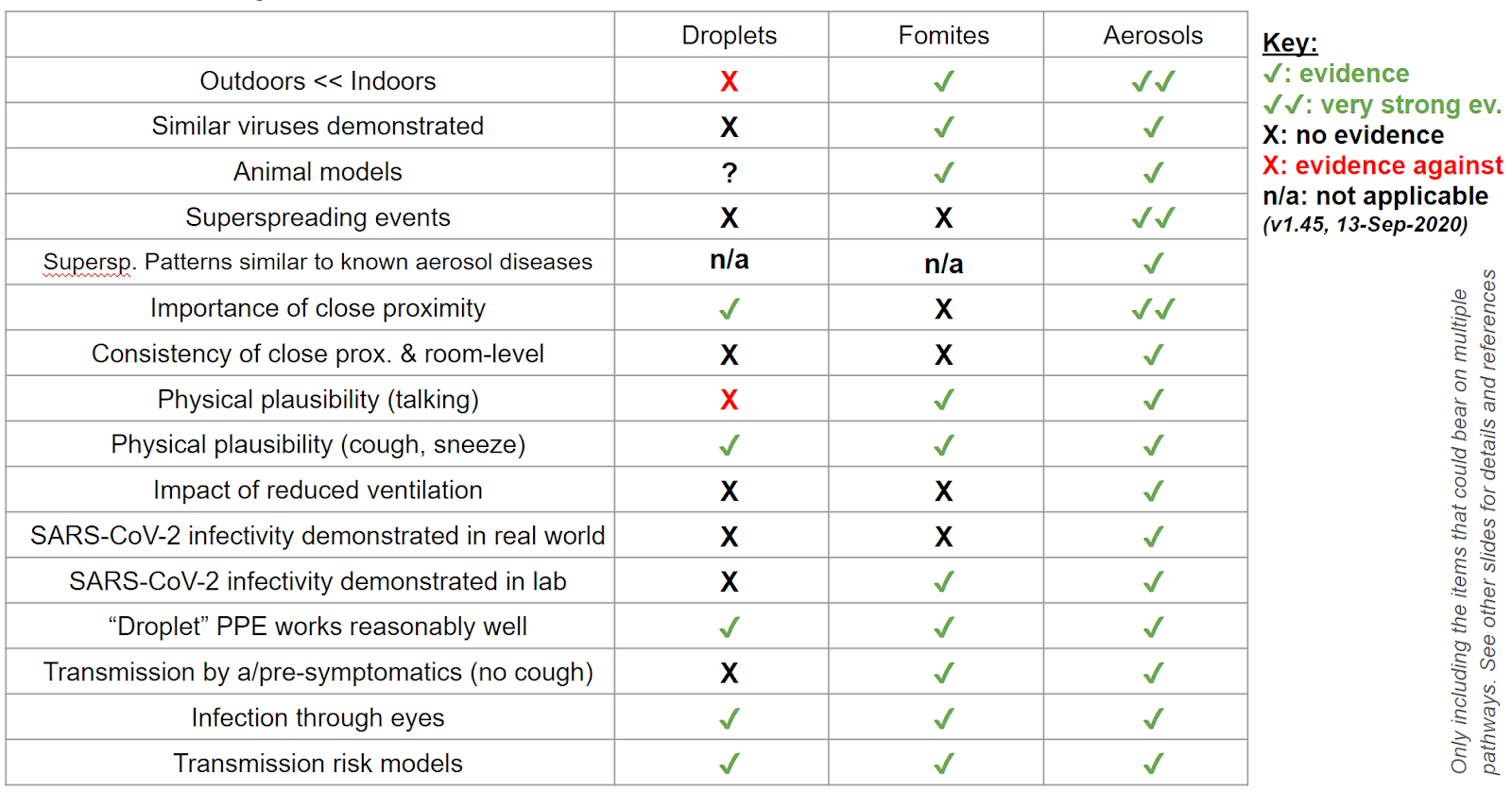
Table: preliminary summary of the evidence supporting each of the three routes of transmission. Aerosols has the most supporting evidence. Fomites has significant supporting evidence. Ballistic droplets have very little supporting evidence.
1.3. But if COVID-19 was transmitted through aerosols, wouldn’t it be highly transmissible like measles, and have a very high R0 and long range transmission?
In a word, no. This is a myth. Here some people are confusing an artifact of history with a law of nature (see also the next question which explains the history in more detail). There is no reason that nature can only produce highly transmissible aerosol-transmitted diseases. It was the entrenched resistance against aerosol transmission initiated in 1910 by Chapin's book on The sources and modes of infection that led to only highly transmissible viral diseases being accepted as being transmitted through aerosols, because only for those the evidence was too obvious to be denied (plus tuberculosis, which is less transmissible, due to some amazing experiments). Other diseases such as the flu, SARS, or MERS also have an aerosol transmission component, but the lack of acceptance of that fact has deprived the medical community of accepted examples of less transmissible aerosol diseases.
Also note that Rt for SARS-CoV-2 is very high for superspreading events, which can only be explained by aerosols. This is easily explained by aerosol transmission, depending on whether infected people participate in situations conducive to superspreading, and with variable emission of viable viruses in time and among people. This leads to a very skewed distribution of R, with many low values, and some very high values.
In addition, measles and tuberculosis were classified as spreading by droplet / fomites for decades. For example this article on measles from 1985 states "Most public health authorities believe that the primary mode of transmission is by large respiratory droplets" and that it "requires close contact." But there were suspicious patterns, e.g. tuberculosis outbreaks occurred in ships, buses, poorly ventilated rooms, and bars (does that sound familiar?). It was later demonstrated that tuberculosis can only be transmitted through aerosols, and that measles is very efficiently transmitted through aerosols. The lesson that we should learn from this history is that it is very difficult to determine the mode of transmission of a respiratory disease, and that often in the past an observation of efficient infection at close proximity (and that social distance works to reduce infection) has been incorrectly interpreted as evidence for droplet and against aerosols. In reality transmission in close proximity is actually strong evidence of aerosol transmission, especially in the absence of cough (which is very relevant to COVID-19 where people where no or few symptoms spread the disease efficiently).
1.4. When you say that the resistance to aerosol transmission is rooted in history, what do you mean?
There is a huge bias embedded in the field of medical infectious diseases since around 1910. It is assumed that droplet infection is obvious and thus needs no strong evidence. For example, it was assumed to be major for SARS-CoV-2 despite a near complete lack of evidence, which continues to this day. On the other hand it is assumed that aerosol infection is extremely unlikely. Since "extraordinary claims require extraordinary evidence," aerosol transmission continues to be downplayed or minimized despite overwhelming evidence that it is much more important than droplet transmission for SARS-CoV-2.
The bias originated with the work of Dr. Charles Chapin, and in particular his seminal book in 1910, The sources and modes of infection. Chapin was a very influential public health researcher, and e.g. served as the president of the American Public Health Association in 1927. In his book he reviewed 50 years of accumulated evidence (since germ theory was demonstrated by Pasteur in the 1860s) about how germs were transmitted for various diseases, e.g through air, water, hands, food, soil, etc. He realized that respiratory diseases were transmitted most easily in close proximity, and that social distance reduced infection (he calls it “contact infection”, but often actual contact is not required, so we prefer to discuss it as “infection in close proximity”). That is an empirical observation, which is correct. It is the reason why we socially distance ourselves to avoid COVID-19 infection, and it has been shown to work very well against many respiratory diseases. Chapin was very successful in applying those principles in his new hospital in Providence, which helped increase his influence in the field of Public Health.
Chapin then tries to explain why social distance works to reduce infection in close proximity. He correctly reviews the two possibilities:
(a) either the infection is transmitted by large droplets that lead to infection by impact on a susceptible person, but otherwise land in the ground. He calls this "sprayborne infection." There was some limited evidence of droplets carrying germs and falling close to the person, from the work of Carl Flugge in Germany in the 1890s.
(b) Or the infection is transmitted through smaller aerosols that float in the air. These could reach further, and it was feared at the time that they could reach huge distances such as crossing the Atlantic, having an infected person in the US transmit influenza to someone in Europe after air travel of the pathogen across the Atlantic Ocean. The older “miasma theory” still lurked in the public consciousness, that diseases were transmitted by “bad air” over considerable distances. At the time respiratory aerosols had not been measured, as they are smaller and much more difficult to study than droplets. In fact it took several decades before respiratory aerosols were studied in detail.
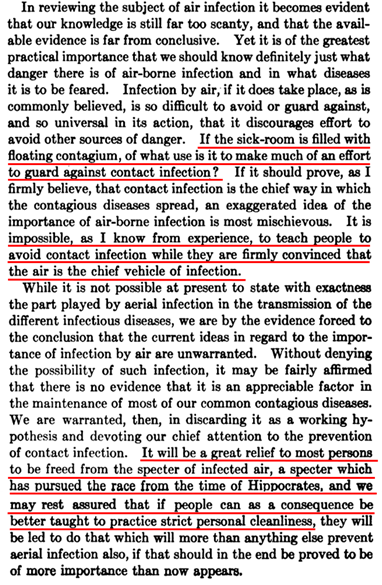
Chapin realizes that it has to be (a) or (b). At the end of the chapter in airborne infection (a highly recommended read, screenshot of critical text below) he admits that he has no evidence to rule out (b), i.e. aerosols. E.g. Chapin wrote “In reviewing the subject of air infection it becomes evident that our knowledge is still far too scanty, and that the available evidence is far from conclusive.” But he also stated that "it is impossible, as I know from experience, to teach people to avoid contact infection while they are firmly convinced that the air is the chief vehicle of infection." Based on that (and other weak evidence where pathogens had not been detected in exhaled air, with methods of the early 20th century) he takes the position that ease of infection in close proximity is explained by spraying droplets, and that aerosol infection is almost impossible: “we are warranted to discard [aerosol transmission] as a working hypothesis” and “It will be a great relief to most persons to be freed from the specter of infected air.”
Thus a fateful error was made without evidence, that sprayborne droplets are the explanation of ease of infection at close proximity (and of why social distance works), and that we can rule out aerosol transmission. Chapin was extremely influential, and his hypothesis became (still without evidence) the paradigm of respiratory disease transmission. Later becoming a dogma, whose origin seems to be lost in the fogs of time, but which had unquestioning adherence by most in those professions. This same error is still being made today, and pretty much for the same reasons, by WHO and CDC. E.g. recently, Tom Frieden, former head of the CDC, made the same error on Twitter, stating that ease of infection in close proximity led to a “consensus” that droplets caused the majority of transmission of SARS-CoV-2. No doubt coming from the same tradition, and once again, ignoring aerosol science as being needed for any such consensus.
Figure: screenshot from Chapin’s book “The Sources and Modes of Infection” (1910). This text is at the end of the chapter on airborne transmission. Red underline draws attention to critical parts, although the whole page is important. |
The droplet paradigm is satisfying and worked well enough during the 20th century for infectious disease control, especially aided by vaccines and pharmaceuticals. Many diseases have an aerosol transmission component, but most are not very contagious. Aerosols are most concentrated in close proximity, about 100 times more than when diluted into a room, so aerosol transmission indeed occurs mostly in close proximity. Suspicious outbreaks that suggest aerosol transmission were dismissed, being attributed to unidentified close contact, poorly used PPE etc. Williams Wells, Richard Riley and others spent much of the 20th century showing that indeed aerosol transmission was possible. However, they encountered fierce resistance as Chapin’s paradigm had taken a firm grip on the field, and they were accused of “bringing back miasmas.”
For many decades, tuberculosis (TB) was described as a droplet/fomite disease (based especially on ease of transmission in close proximity), despite suspicious outbreaks in ships, bars, buses, choirs, poorly-ventilated rooms (sounds familiar?). Finally, the spectacular Wells-Riley experiments of the 1950s make it undeniable that TB can be transmitted through aerosols. It will later become clear that TB can only be transmitted through aerosols, as the pathogen needs to reach the alveolar macrophage in the deep lung, which only small aerosols can do.
A similar story played out for measles and chickenpox. Although today measles is described as the prototypical highly transmissible aerosol disease, as recently as 1985 “most public health authorities believed that the primary mode of transmission is by large respiratory droplets which remain suspended in air for short time intervals. Successful transmission in this manner requires close contact between susceptible individuals and a source patient, usually within 1 m (3 ft.)” Evidence supporting this view included anecdotal evidence of lack of transmission in some hospitals with measles patients, (which is the same argument made by the WHO IPC committee to deny aerosol transmission of SARS-CoV-2).
Other diseases such as the flu, SARS, or MERS also have an aerosol transmission component, but the lack of acceptance of that fact has deprived the medical community of accepted examples of less transmissible aerosol diseases. Leading to an artifact of history (only highly transmissible diseases have been accepted as being transmitted through aerosols, less transmissible ones have been denied) being confused with a law of nature (all aerosol-transmitted diseases need to be highly contagious, which makes no sense whatsoever).
1.5 Are all infected people equally contagious?
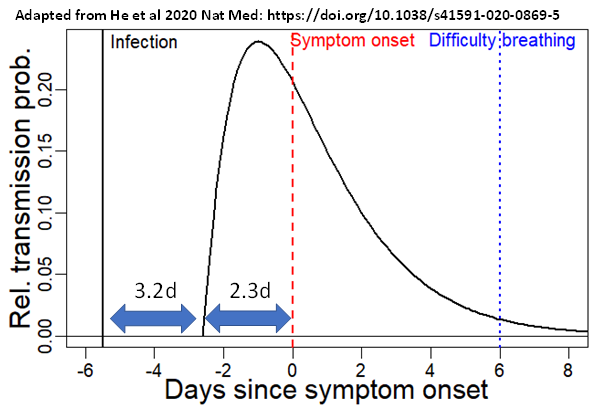
Not at all. First of all, it is very clear that there is a large variability in time for a given person. It is very well known that there is a peak of contagiousness just before and at the onset of symptoms, and that then contagiousness decreases (figure below). By the time most people are sick enough to go to the hospital, many are not contagious. In addition, even for infected individuals virus emission is not constant, but it is rather an sporadic event. Unfortunately a lot of data is interpreted as if contagiousness was constant during the disease, even by key experts on WHO’s own committee. This leads to a lot of misinterpretation and confusion.
Figure: relative probability of transmission of SARS-CoV-2 from an infected individual as a function of time in the disease. The peak of infectiveness is just before the onset of symptoms. Reference: Prof. A Marm Kilpatrick, University of California-Santa Cruz. |
In addition, it is likely that some individuals are more contagious than others. This can be due e.g. to higher viral load at the onset of symptoms, to higher emissions of respiratory particles, or (likely) to both. It is known that some people exhale 10 times more aerosols when speaking, although the reason is not understood. This variability likely helps explain the high dispersion in R (many people don’t transmit the disease to anyone, but a few lead to superspreading events) and the relatively low attack rate in households. I.e. some infected people don’t exhale much virus, while others exhale a lot for a few days.
1.6. So should I keep washing my hands and being careful about elevator buttons, light switches, door knobs etc?
Yes! While we think that aerosol transmission is more important than this “touching” (fomite) route, there is evidence that the virus can be transmitted in this way. So you should keep washing your hands, using hand sanitizer etc. But you should pay at least as much attention to the air you breathe as you do to sanitizing surfaces and your hands.
1.7. Where can I find more scientific information at a higher level about aerosol transmission?
A great source is the 11 hr recording of the recent Workshop on Airborne Transmission of SARS-CoV-2 from US National Academies of Science, Engineering, and Medicine (the highest level scientific body in the US). The workshop was co-organized by two of the writers of these FAQs (K. Prather, L. Marr), and two others spoke in it as well (S. Miller, C. Haas).
2. General questions about aerosol transmission
2.1. What is aerosol transmission?
When we talk, shout, sing, cough, sneeze or simply breathe, we exhale small particles (“aerosols”) that are made of saliva or respiratory fluid (the liquid that wets the inside of your trachea, lungs etc.). These aerosols are the “carriers” of SARS-CoV-2 viruses, and can infect when they are inhaled. See more detail and a figure above.
2.2 What is the size of infectious aerosols?
While the size of an individual SARS-CoV-2 virus is very small (120 nm or 0.12 microns), the aerosol in which respiratory viruses are contained are larger, albeit still small enough to remain suspended in air for long periods. A widely held misconception is that the virus is naked in the air, perhaps with some water. This has been propagated by graphics in major medical journals such as JAMA. Our best guess is that the most common aerosol size is a few microns, where the viruses comprise a very small fraction of the aerosol, as exemplified in the figure below. Aerosol size has major implications for the ability of masks and filters to remove it from the air, how deeply it will penetrate the lungs, and determines the loss rate due to gravitational settling in indoor spaces.
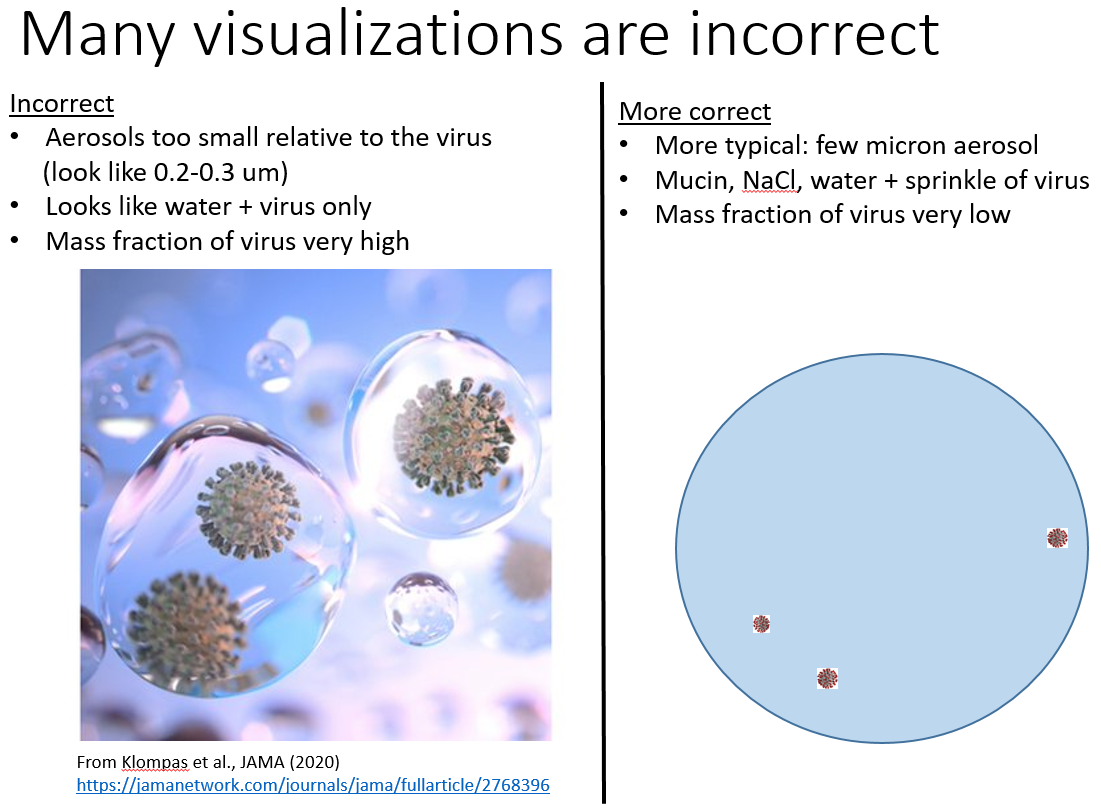
Figure: visualization of the virus in aerosols. Left: the most likely incorrect representation of the virus as naked in the air, containing only some water. Right: a likely more correct representation, with the virus accounting for a small fraction of a larger aerosol.
The size distribution below (link) represents the typical number of aerosols as a function of size, as they come out of a person (blue, high amount of water) and as they dry under typical ambient conditions.
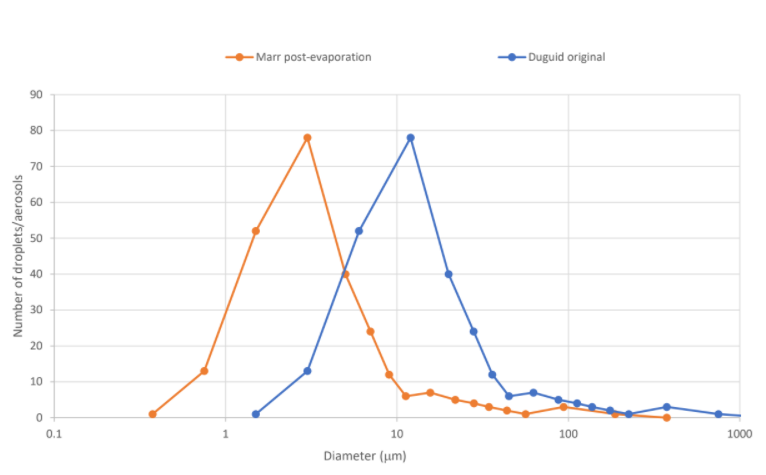
Figure: Distribution of the number of aerosols and droplets emitted from a person counting from 1 to 100 vs. particle size. The blue distribution included a large amount of water from the respiratory tract. The orange distribution accounts for the drying that occurs when the aerosols dilute in typical ambient environments.
The figure below shows more recent data, in a logarithmic vertical scale (which makes it much harder to interpret for people who are not used to reading such graphs). The
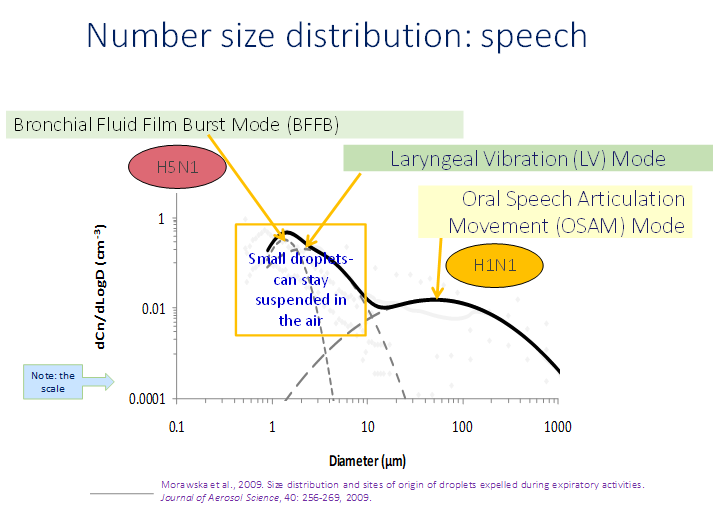
Figure: size distribution of aerosols and droplets produced by speech, indicating the three “modes” in size, each of which is attributed to a different production mechanism. The smallest aerosols come from deep in the lungs, the intermediate aerosol mode from the vocal chords, and the largest aerosols and droplets come from the mouth during speech. From the presentation of Prof. Lidia Morawska to the National Academy of Sciences, Engineering, and Medicine. Note that this is a number distribution, and that the volume increases with the cube of the particle size.
2.3 What factors control how many infectious aerosols are exhaled?
See question above for variability in time and between people.
In detail, the sizes of the aerosols and the amount of the virus exhaled vary with the stage of infection and from person to person. They also vary with individual activity, with many fewer from breathing and many more from talking, singing, shouting and (very likely) aerobic exercise. There is evidence that a combination of these factors and the venue where the emission occurs can result in “superspreading events”. The aerosols stay floating in the air for minutes to hours. If another person inhales them, they can become infected and then later infect others.
2.4. Where do aerosols of different sizes deposit in the human respiratory tract?
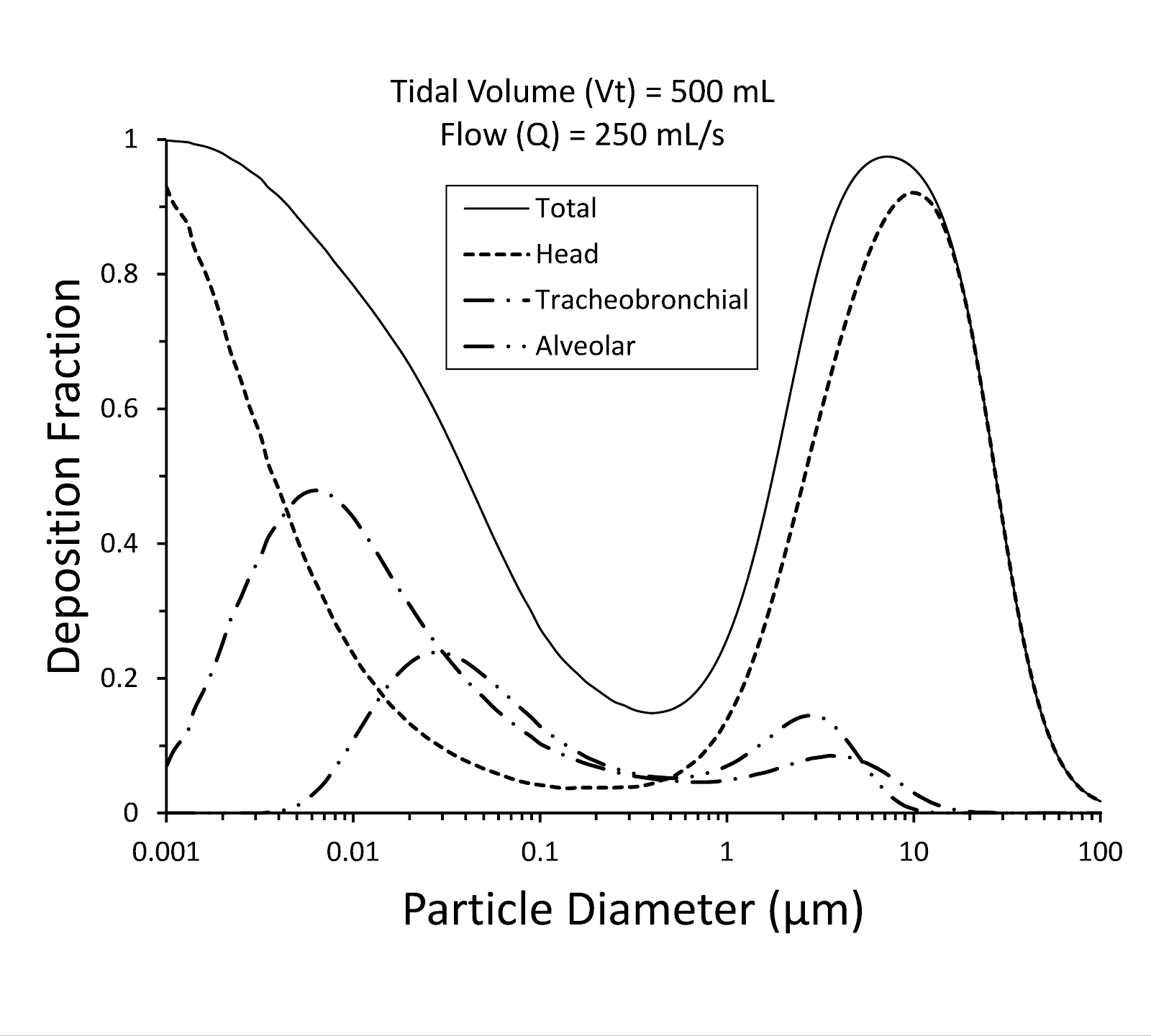
The figure below (from US EPA) shows this information graphically. Particles smaller than 100 μm can be inhaled (i.e, are aerosols), while larger particles cannot (and they are “droplets” in the disease transmission sense).
Of the aerosols that are inhaled, many deposit in the respiratory tract, but many do not (black line on top). In particular there is a minimum at 0.3 μm, which is the typical size of smoke aerosols. This is why smokers exhale a lot of smoke aerosols; not all of them deposit in the respiratory tract, so some come back out in exhaled breath. Thus even though masks are least efficient at blocking aerosols of size 0.3 μm, the same physics (that causes masks to be less efficient at this size) means that it is also less likely for those aerosols to deposit in our bodies.
Larger aerosols deposit in the head region (nose etc.) because they can’t make turns easily, and impact with the walls of our nasal and oral cavities. As the size approaches 100 μm, the aerosols are “clumsier” and thus less likely to follow air flow into our noses and mouths, and settle to the ground faster, so the efficiency of inhalation becomes very low. Very small aerosols are very diffusive (i.e. high brownian motion) and are also lost efficiently in the head region.
Aerosols smaller than ~10 μm can penetrate deeper into the respiratory tract. But it is important to note that aerosols smaller than10 μm can deposit everywhere along the respiratory tract, and viruses contained in them can reach receptors anywhere in that tract.
Figure: fraction of inhaled aerosols that are deposited in different parts of the human respiratory tract (from US EPA). |
2.5. Some people say that “aerosols” vs. “droplet” transmission is a semantic discussion, and that both can infect by inhalation. Is that correct?
The most important definitions are those of WHO and CDC, because the recommendations for protection are derived from them. Also the physical understanding arising from them is used by many people as they think about protecting themselves in their own specific situations. Most countries do not have a strong CDC-type body that would be confident in contradicting WHO. Many scientists around the world report that speaking out against WHO’s recommendations is simply not possible in their situations.
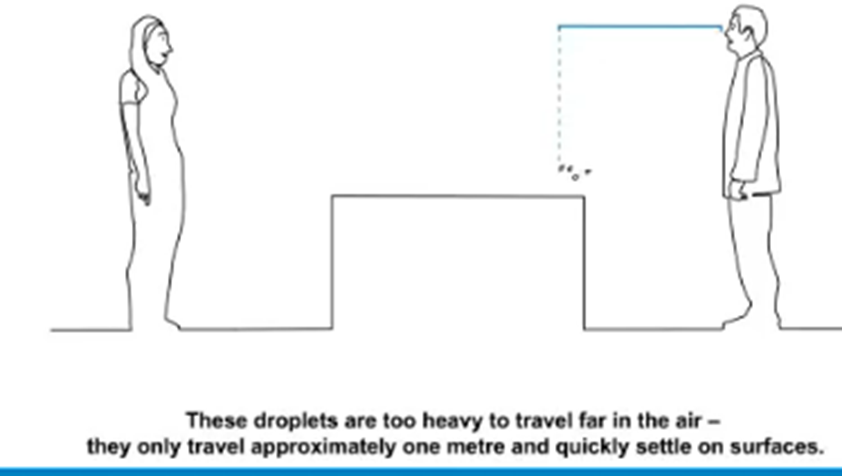
As exemplified by their own graphics below, they both define “droplets” as projectiles that infect by impaction and fall quickly to the ground (we often call them “ballistic droplets” to make this behavior clear). And aerosols are particles that remain in the air for minutes to hours and infect by inhalation.
Figure: still from a WHO video showing ballistic droplets flying from a person’s mouth and falling within 1 m of the person. This particular image shows why social distance works, as it eliminates the chance of impact on the susceptible person’s eyes, nose or mouth. |
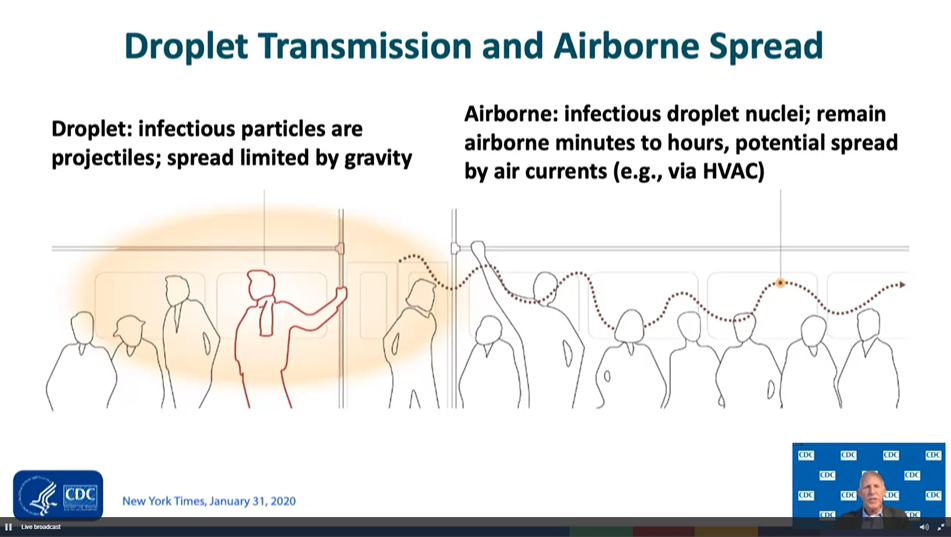
Figure: slide from Dr. Butler from the CDC during the recent NASEM workshop on airborne transmission of SARS-CoV-2. Droplets vs. aerosols are clearly defined. |
These definitions are reflected in their guidelines, for example WHO’s website still only recommends masks indoors if a social distance of 1 m cannot be maintained. This logically follows from infection being caused by ballistic droplets that land within 1 m of the person.
Some scientists and others say that this is semantics, and describe “droplets” that are not ballistic, but that have aerosol behavior, persisting in rooms with low ventilation, and infecting by inhalation. This is often used to explain outbreaks that can really only be explained by aerosols, while still maintaining they were caused by “droplets.” Also CDC states that droplets “can possibly be inhaled into the lungs,” which is not possible for ballistic droplets (see below). And measures like ventilation are recommended by WHO and others, despite asserting that it is ballistic droplets and not aerosols that dominate transmission. These two statements are contradictory, as ventilation has a minimal effect on ballistic droplets, but it does have a large effect on aerosols.
There is a clear distinction in size between ballistic droplets and aerosols, thus this dichotomy is very useful:
- Particles smaller than ~ 100 μm do not settle very quickly to the ground, do not have enough inertia to reach others as ballistic droplets, and can be inhaled. These can only infect as aerosols.
- Particles larger than ~300 μm (see also here) have enough inertia to reach someone else at 0.5-1 m distance (typical US conversational distance) when talking, which is most relevant for SARS-CoV-2 where much transmission occurs for people with little or no symptoms who don’t cough. These are the only possible ballistic droplets. Note that the widely used definition of > 5 μm for ballistic droplets is completely wrong, and has been for decades, as discussed below.Thus there is a “valley of death” between 100 and 300 μm where particles typically cannot infect as aerosols or ballistic droplets (when talking at typical distances). Particles of those sizes are unlikely to participate in infection, except for coughs and sneezes where the stronger exhaled momentum propels them farther, or by deposition and the fomite route.
For those particles that infect as aerosols (<~100 μm), there is a huge accumulated body of knowledge about how to control them (as exemplified by these FAQs). Describing aerosol behavior but calling it an extension of droplet behavior is confusing, and leads to unclear guidelines, not allowing people to efficiently protect themselves from transmission. And it also reduces the pressure on WHO, CDC, and other agencies to acknowledge aerosol transmission as being as important as the other routes. If scientists use the term “droplet transmission” to e.g. explain an aerosol-driven outbreak (e.g. the Skagit choir), they appear to agree with WHO and CDC that transmission is dominated by ballistic droplets. Thus no changes in the description of the transmission routes and their importance, or in the recommendations, are needed. But this is very misleading if the term “droplets” is being used to describe aerosol behavior: particles that stay in the air more than a few seconds, that do not fall to the ground in 1-2 m, and that infect by inhalation. Such misleading use of the terminology is making progress on this issue more difficult.
2.6. But many documents define aerosols as smaller than 5 μm and ballistic droplets as larger than that size. Is that incorrect?
Yes, it is a huge error, which has been repeated by major institutions and countless scientific papers for at least 3 decades. Several authors of these FAQs are working on a manuscript documenting how and when the error occurred and what caused it, which will be available as a preprint in the near future.
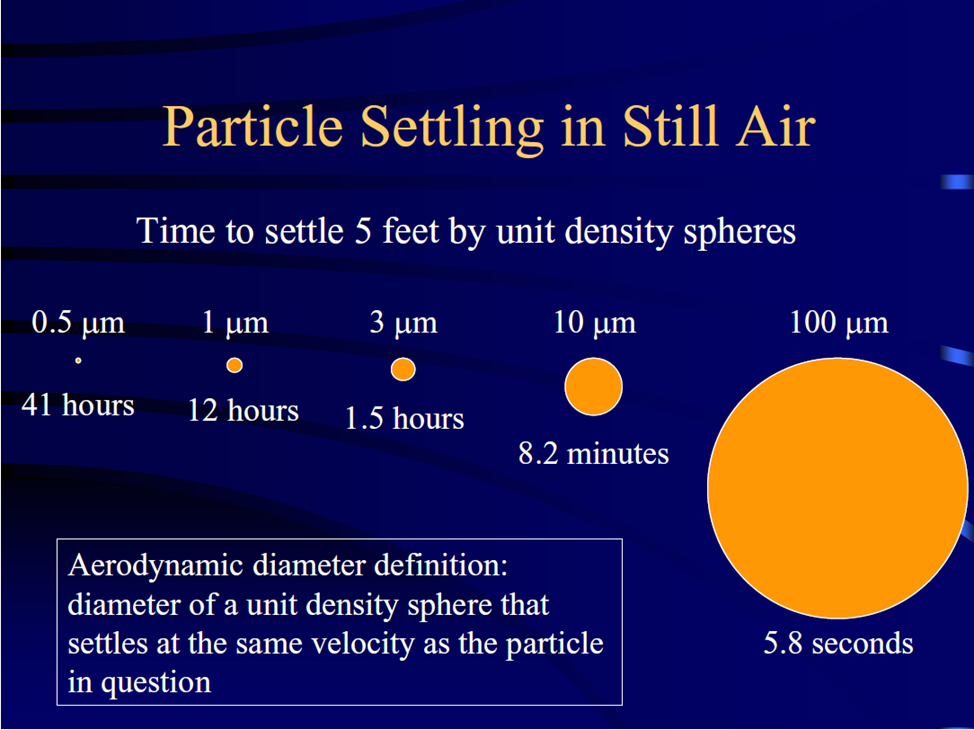
The real boundary between ballistic droplets and aerosols is ~ 100 μm, as discussed in the recent NASEM workshop. This has been known at least since Wells (1934). Or the slide below, from the CDC website, that shows that aerosols ~10 μm in size can stay in the air for 8 minutes, and thus do not fall to the ground in a few seconds. At typical indoor air speeds of 0.1 m/s, a 10 μm aerosol can travel ~50 m.
But for ballistic droplets to have enough inertia to be able to reach others when talking, they need to be >300 μm (see also here). Motion is determined by mass (F = ma), and WHO and others are making an error of a factor of 200000 in the mass of ballistic droplets! An important consequence is that ballistic droplets are far less numerous than they assume, which greatly reduces the probability of infection by ballistic droplets when talking.
Figure: time for particles of different sizes to settle to the ground in still air, from the height of a person. From the CDC “Aerosols 101” presentation. |
Dr. Anthony Fauci has acknowledged this error on 10-Sep-2020, stating: “The aerosol physicists have approached us now have told us that we really have been wrong over many many years and that particles greater than 5 microns still stay in the air much much longer than we had thought, when we used to say empirically greater than 5 microns it drops to the ground, and 5 microns this might be aerosolized, we know now this just not the case.”
2.7. How long does the SARS-CoV-2 remain infectious in aerosols?
Multiple studies have addressed this question in the laboratory (see here, here, and here). Overall it seems that the lifetime may be about 1-2 hours at typical room temperature (~20oC or 70oF). When coming to an office in the morning at 8 am when people left the previous day at 5 pm, any viruses in the air will have been ventilated, deposited, or lost infectiousness. For this reason it is a good idea for high-risk people to go to indoor public spaces as soon as they open in the morning.
2.8. Does temperature affect the survival of the virus in the air?
Low temperatures can greatly increase the survival of the virus, while high temperatures reduce it. Superspreading events in meat packing plants are thought to have been helped by higher virus survival in the air at low temperature. Researchers freeze viruses to keep them viable for years, although this requires lower temperatures than in home freezers (-80oC). Higher temperatures reduce the viability of viruses. Humidity also has an effect that cannot be easily separated from that of temperature, as discussed below.
2.9. Does relative humidity (RH) affect transmission?
Humidity has a few effects:
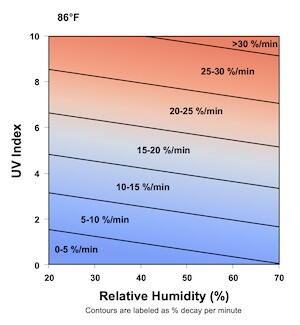
- Lipid-enveloped viruses, including SARS-CoV-2, are thought to survive better in the air under drier conditions. The graph below is from the US Dept. of Homeland Security online calculator. This is thought to be an important reason leading to the flu season in winter, as indoor air is drier then.
- Dry conditions may also make humans more susceptible to infection, due to factors such as epithelial damage, mucociliary clearance impairment, and increased mucin
production.
- Respiratory particles contain an amount of water that depends on the ambient relative humidity. However aerosols dry in less than 1 s. As was well put by Wells (1934), because of the way the physics works out, “a raindrop 2 mm in diameter can fall miles without completely evaporating under conditions which would cause a 0.2 mm [= 200 μm] droplet to evaporate before it had fallen the height of a man.”
- If the humidity is larger than ~85%, aerosols are larger than at lower humidity and thus the growth due to water uptake makes them settle faster to the ground. At lower humidities this effect is very small.
- This only matters for shared room (and any potential long range) transmission, if the distance is not kept, transmission in close proximity is not impacted by humidity or temperature.
Figure: decay rate of the viability of SARS-CoV-2 virus as a function of relative humidity and UV light. From DHS calculator |
For more details on these effects, see Ahlawat et al. (2020). There is also some discussion that an intermediate humidity in the range 40-60% may be beneficial to reduce virus viability, based on past studies with other viruses. However, the medium in which the virus is aerosolized has a strong impact on its survival. Some of those studies were performed with culture media, instead of more representative fluids like simulated saliva. So our impression at present is that while preventing low humidity indoors can be useful, the benefits of keeping it in the 40-60% range are less clear.
See also the question below about humidifiers and dehumidifiers.
2.8. Is there an analogy for aerosol transmission?
Second-hand smoke (or vaping) is the best analogy. We are all used to seeing, and smelling, other peoples exhaled smoke, and know that smoke does not fall to the ground quickly. It is most concentrated right in front of the smoker, and then it is mixed by air currents. In a room with low ventilation, it can build up. In most indoor environments, a small fraction, e.g., less than 10%, will deposit on indoor materials and the remainder will stay airborne until exhausted to outdoor air.
Now, the virus-containing respiratory aerosols are not visible, because there are far fewer of them than for smoke. But they behave in the air in the same way because they have the same sizes. So you can imagine that others are exhaling smoke, and you want to breathe in as little smoke as possible, especially without a mask. That is how you can reduce your chance of infection.

Figure: Left: visualization of exhaled smoke. Concentration is highest in front of the smoker, much lower elsewhere in the room. Right: smoke level can build up in the room, if there is low ventilation, a long time etc.
This analogy allows people to think about how to protect themselves, and we will use it in other FAQs. That said, it is not perfect and its behavior departs from that of the virus in several ways:
- Smoke contains aerosols (that we can see) and gases (that we can smell). Aerosols are filtered by masks, but gases are not. The fact that the smell penetrates the mask does not mean that the mask is not filtering the aerosols.
- Smoke can linger in clothes, walls etc. far longer than the virus can stay infective.
- For vaping, aerosols are formed from evaporation and condensation of vapors (i.e., gases). The gases can traverse the mask, and then condense and form aerosols when they mix with cold air just outside the mask. Aerosol scientists use this process routinely in the laboratory. Some videos online purport to show that masks don’t work based on this misconception, in addition to 2 other misconceptions: masks are known to have the lowest efficiency at ~0.2 microns, which is the size of vaping aerosols. With a huge source, even a mask that’s 80% efficient will let through enough aerosols to form a visible cloud. This does not mean that the mask is not working, the mask is still capturing 80% of the aerosols! To say that a mask doesn’t work because some aerosols can penetrate it is like saying that a coat doesn’t work to protect ourselves against the cold, because some heat still escapes through it. And in addition, mask fit is critical, and most of the masks in that video show very poor fit.
2.9. Does that mean that smoking can help spread the virus?
Smoking can increase the emission of viruses into the air, because smokers have to remove their mask to smoke, and because they may breathe more forcefully.
In terms of smoke particles carrying the virus, we think this is very unlikely. Smoke is simply an analogy to visualize the motion of the virus. Smoke does not lead to greater aerosolization of virus from the respiratory tract. Once the virus is aerosolized, it could stick to smoke aerosols as they all exit the nose or mouth together, but the virus would have come out into the air anyway.
Smoking and vaping destroy cilia in your respiratory tract. These are responsible for removing viruses out of your system and protecting you from infection. But they are also where the ACE2 receptors that the virus uses for infection are located. Thus it is observed that smokers are less likely to be infected by COVID-19. But if they are infected, according to CDC, smokers may be at higher risk for severe illness from COVID-19.
2.10. Can pollution aerosols help spread the virus?
Not that we know of. There was an Italian article, and a lot of discussion online, about whether the virus could attach itself to pollution aerosols and travel farther that way. This hypothesis builds on the misconception that viruses are naked in the air. They are not.
Pollution aerosols are mostly ~0.3 μm, which is much smaller than the sizes that are thought to dominate SARS-CoV-2 transmission (~3 μm). If a pollution aerosol (relative size of a cat) attaches to a virus-containing aerosol (relative size of an elephant), the elephant doesn’t notice.
There was also a lot of speculation early on about air pollution enhancing transmission because the pandemic spread earlier in more polluted places like Lombardy or Madrid, which are very polluted. However, it seems that the pattern can be more easily explained by those regions also having much higher travel with China and internationally, and thus the virus arriving there earlier. Then the virus arrived later to rural areas, but it spread there just as well.
What appears more likely are interactions similar to those described above for cigarette smoke: smoke causes problems in the respiratory system of people who live in polluted areas, and that can potentially change the probability of infection in a given situation, or the severity of the disease.
3. Protecting ourselves from aerosol transmission
3.1. At what distance from an infected person can I get infected?
There are three relevant scales. Note that these terms are not used consistently across scientific disciplines.
- “Close proximity,” < 1-2 m
- There is a lot of COVID-19 transmission in close proximity situations. But it is not 100% efficient. As we understand from contact tracing, some close proximity encounters do not lead to infection.
- “Shared room,” sharing the air of the same room at the same time
- Clearly there is aerosol transmission in shared rooms, as has occurred in many superspreading events. But a very clear pattern emerges, that indoors is needed for superspreading, and it is helped by long time, crowding, low ventilation, no masks, and talking and especially singing / yelling. E.g. lots of outbreaks occur in choirs / bars / meat packing with high attack rates, but none have been reported (to our knowledge) in Japan's subways, or in movie theaters where there is almost no talking and better ventilation. As one would predict with the smoke analogy or a mathematical model.
- “Long-range,” when not in the same room, e.g. different rooms in the same building with some air through HVAC, or entering a room 2 hrs after someone infectious has been there etc.
- There are no documented cases that we are aware of. This is consistent with the expectation for a generally less contagious virus.
- Some cases of long-range transmission of COVID-19 are being documented, but they appear to involve fecal aerosols transmitted through the sewer lines of high-rise buildings in Hong Kong and China, and not respiratory aerosols produced when breathing or speaking.
3.2. Do the 1-2 m or 6 feet guidelines guarantee lack of infection indoors?
Like other recommendations, these social distance rules will reduce risk, but not eliminate it. The 6 feet rule is based on the idea that large ballistic droplets fall to the ground within 6 feet, although they can travel farther in a cough or sneeze, up to 28 ft (8.5 m). The 6 feet rule also helps with aerosols that do not settle to the ground because they are most concentrated close to the person who released them, like cigarette smoke is most concentrated close to the smoker. Dilution over distance is the main reason why social distance reduces transmission of COVID-19.
Where will the concentrated aerosols from a person go? It is almost impossible to say. Indoor air is a constantly changing, turbulent environment. Even though you can’t feel it, indoor air is constantly moving (typically between 0.05 to 0.1 m/sec, or 0.15 to 0.3 ft/sec) due to heat from your body (adults typically give off as much heat as an old incandescent light bulb, 75 to 100 W), sunlight warming surfaces, people moving and breathing, and mechanical heating and cooling induced airflows. You likely have seen this when looking at visible aerosols floating in a sunbeam, or when extinguishing a candle indoors. The aerosols rarely are all going the same direction.
This constantly changing environment will dilute plumes of aerosols. The dilution will be greater with more time and space. Hence, the farther away you can be from other people indoors, the better.
3.3. How long does one need to inhale infectious aerosol to be infected?
Catching a whiff of exhaled breath here or there is very unlikely to lead to infection. The amount of time you spend in close proximity or in a shared room with an infected person affects how much virus you actually inhale, which will dictate your risk of becoming infected. There is no clear amount of time as far as we know, but it would seem to be in the order of minutes.
The CDC says that 15 minutes of talking with an infectious person in close proximity is typically needed to get infected. However, that seems arbitrary to us and is not supported by evidence as far as we know. It can also give a false sense of security that a 5 or 10 minute interaction is safe because it is under the 15 min. threshold.
3.4. How long can the virus stay in the air indoors?
How long the virus stays in the air with the capability to infect depends on three processes.
Deposition depends on the size of the droplet/aerosol that’s carrying it, as well as on the amount of clutter and air motion in the room. Virus has been found in tiny aerosols, smaller than 1 micron, and these can stay floating in the air for more than 12 hours, BUT these small aerosols will typically leave a building in the air faster than they settle on indoor surfaces and the virus can decay during this time (see 2.7. How long does the SARS-CoV-2 remain infectious in aerosols…), even if the aerosols carrying it are still floating in the air.
How fast does air leave a room? It is a little complicated. Think about a cup of black coffee. How much milk do we have to add to the cup before we only taste milk? If we add one cup of milk to our cup of black coffee (allowing it to overflow) the result will still be a tan mixture. In fact, due to mixing it will be just two thirds milk. We would need to add three cups of milk to get our original black coffee cup to be 95% milk.
Indoor air behaves the same way. As outdoor air enters an indoor space it mixes with the air already indoors. So how long does it take to replace aerosol laden air from indoor spaces with outdoor air? In residences, 95% of the indoor air will likely be replaced with outdoor air in a time frame that ranges from 30 minutes to 10 hours. In public buildings, 95% replacement may take between 12 minutes to 2 hours. In a hospital, 95% replacement might take 5 minutes.
So how long a virus can stay in the air indoors is highly dependent upon the indoor environment.
3.5. How can I protect myself from aerosol transmission indoors?
We can never be perfectly safe, only safer. Hence, we need to take as many steps as possible to reduce the risk of our activities. You should try to avoid or reduce as much as possible situations that facilitate inhaling the “smoke” (exhaled air) from others. To reduce risk avoid:
- Crowded spaces
- Close proximity to others
- Low ventilation environments
- Long durations
- Places where people are not wearing masks
- Talking, and especially loud talking / shouting / singing
- High breathing rates (e.g., indoor aerobic exercise)
Each one of these features potentially increases the aerosol concentration you might inhale indoors. So if you must enter one of the above situations, complete your tasks as quickly as possible to reduce your exposure duration and risk.
3.6. Is there a way to remember all the things I need to reduce or avoid?
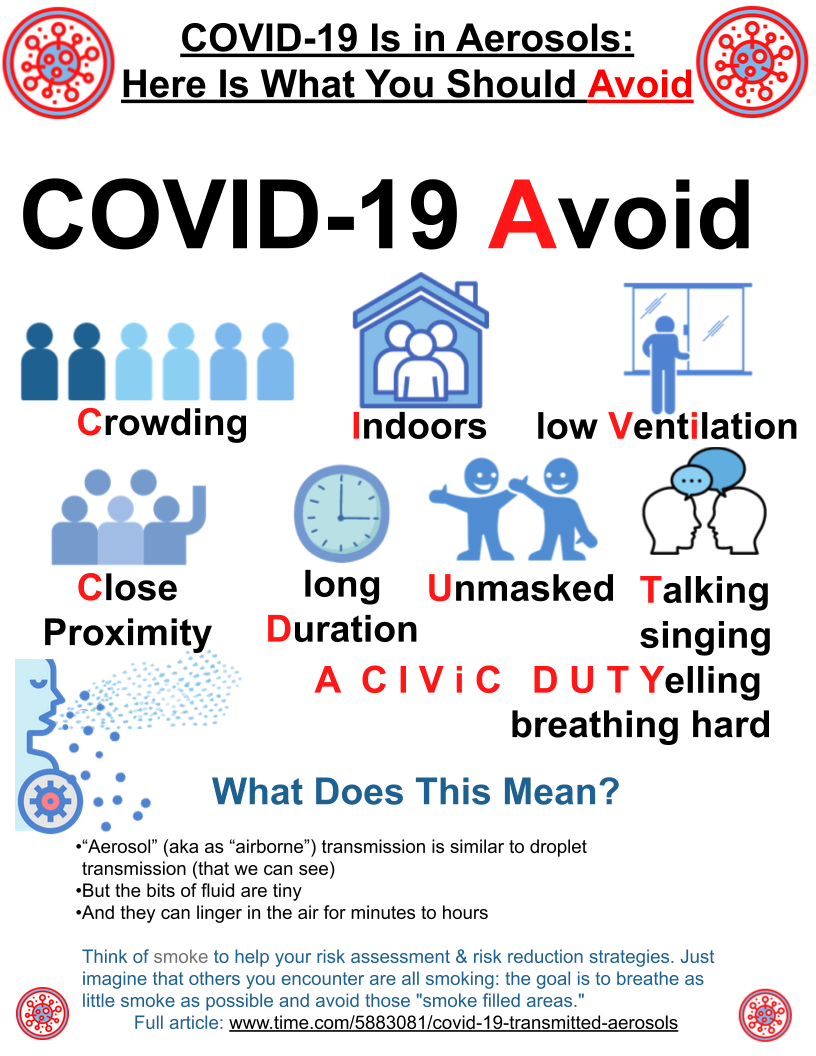
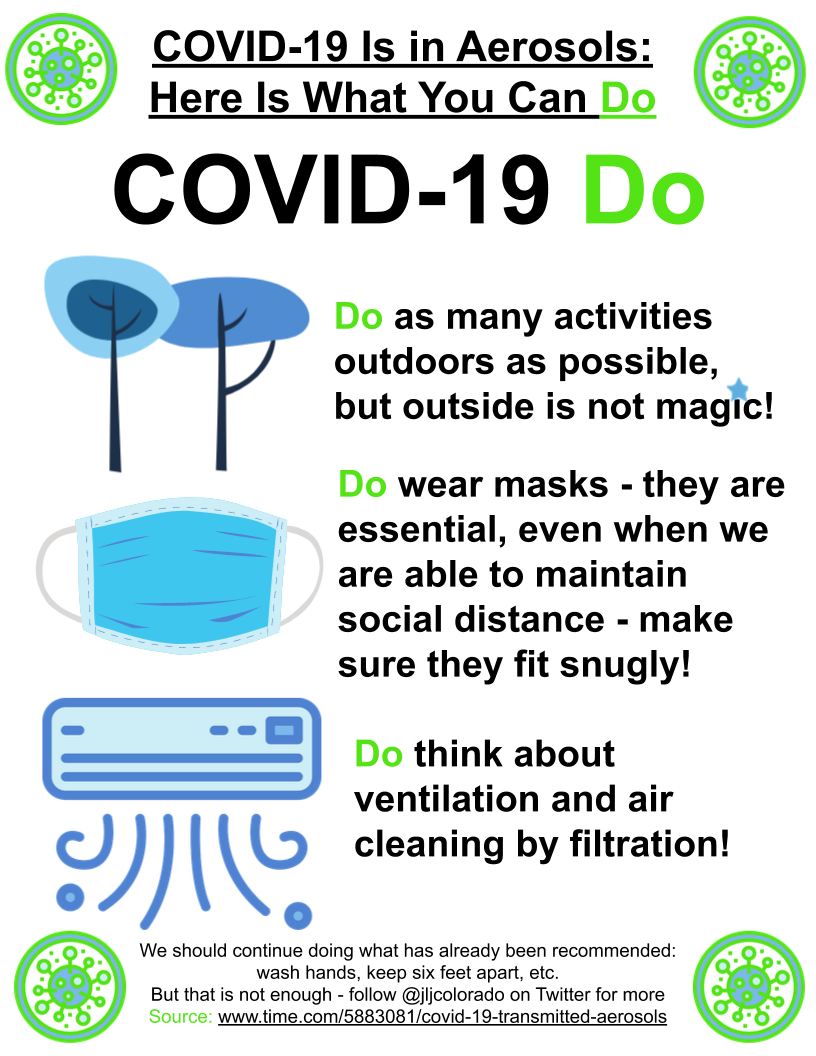
We have proposed an acronym / mnemonic: Avoid Crowding, Indoors, low Ventilation, Close proximity, long Duration, Unmasked, Talking/singing/Yelling/breathing hard (“A CIViC DUTY”). A volunteer made the posters below. There is a lot of room for improvement by creative people on both the acronym and the graphics. A version in Spanish can be found here. To adapt the posters into other languages (or improve the English version), make a copy by clicking on this link and edit away.
glasses
Another series of posters with the same message can be downloaded from here. Examples below for the first couple:
3.7 Aren’t your recommendations the same as Japan’s 3 Cs?
They are similar, but our recommendations encompass several additional items. The 3 Cs recommend avoiding indoors, low ventilation, and crowded situations. But it does not mention avoiding unmasked situations, of long duration, and where talking / singing / shouting / breathing hard.
And if the mechanism of infection (aerosols, like smoke) is not mentioned, people don’t understand such recommendations, and have a hard time following them or adapting them to new situations. In our experience, once people understand “it’s like smoke, and you want to breathe as little smoke as possible”, they very quickly figure out what they need to do in their specific situations.
3.8 Is there a way to understand the relative risk of different environments?
The microCOVID project provides risk estimates for different locations, activities, and personal risk levels.
National Geographic has adapted the aerosol transmission estimator into a simplified online calculator to allow visual estimation of risk under different situations.
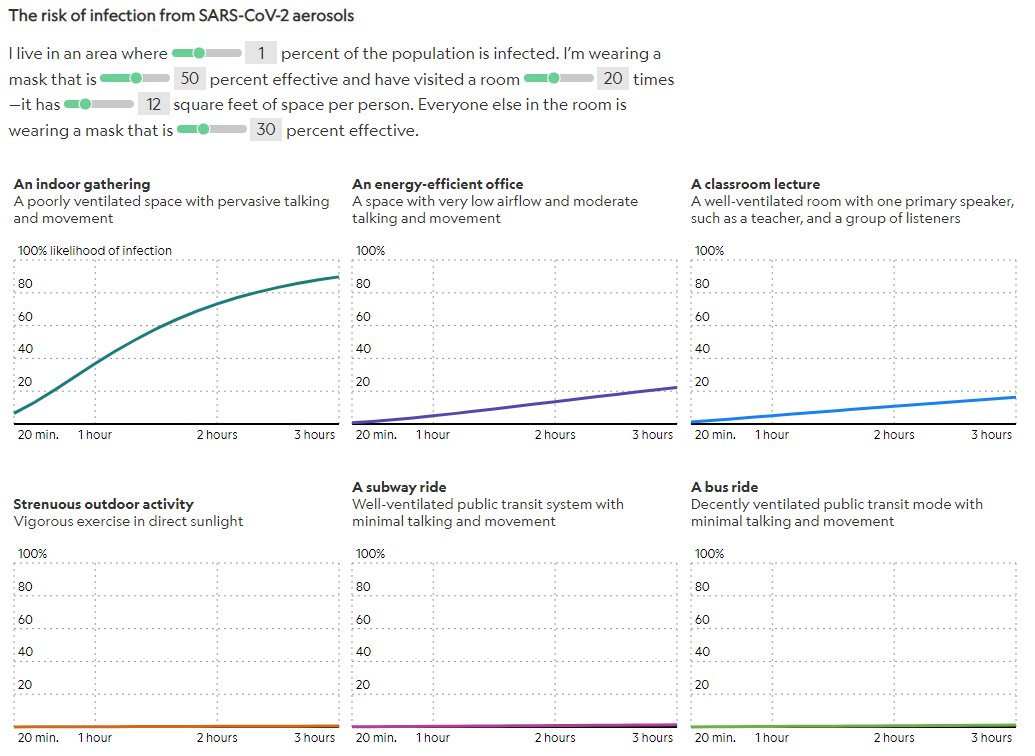
Figure: screenshot from the National Geographic aerosol COVID-19 risk estimator.
The table below has been proposed by Jones et al. (2020). It provides the relative risk of different environments, using almost the same parameters of the “A CIViC DUTY” acronym and the mathematical models.
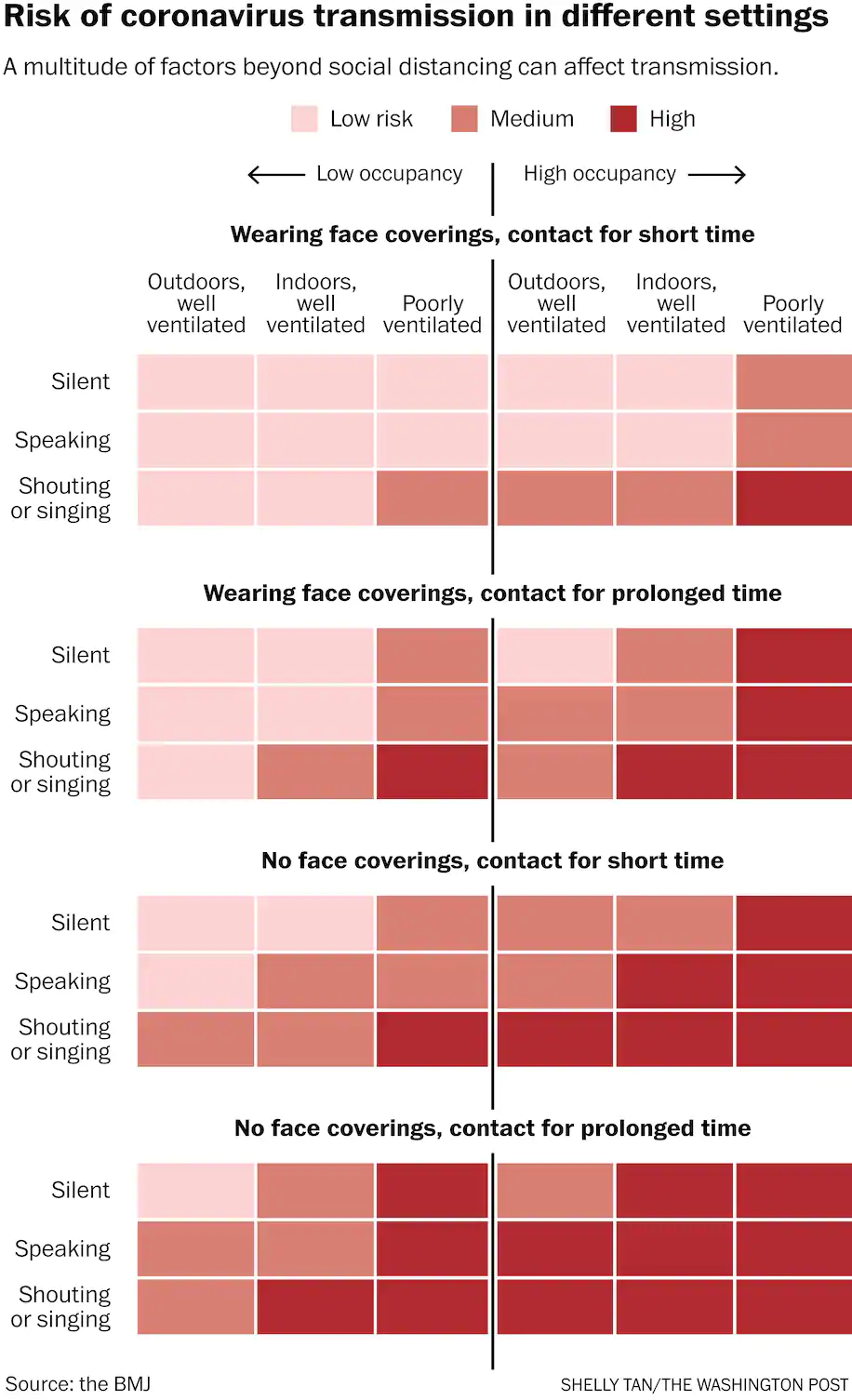
Figure: estimated relative risk of COVID-19 transmission for different activities. Table from Jones et al. (2020), as redrawn by the Washington Post. (We understand that the table is qualitative, and there is some debate about some details. We plan to work in an improved version of this table using the aerosol transmission estimator).
3.9 Is there a more quantitative way to investigate ways to reduce aerosol transmission?
Yes, several mathematical models have been developed that allow you to estimate the risk of infection (with higher uncertainty) and the reduction of risk when doing one or several things (with much better accuracy). One of them is here: https://tinyurl.com/covid-estimator. See the Readme and FAQ pages for extensive information on methods, assumptions, limitations, links to other similar tools etc. It requires some familiarity with math and spreadsheets. If you find it too confusing, find someone who can help (e.g. the science teachers in a school).
Another useful tool is the NIST FaTIMA model. Although it does not estimate the risk of infection, it has more detail to estimate exposure.
Several similar tools have been developed by other researchers, and the publicly available ones we know of are linked in the FAQ page of https://tinyurl.com/covid-estimator.
4. Outdoors
4.1 Is there a risk of aerosol transmission outdoors?
All data show that outdoors is far safer than indoors, for the same activity and distance. But that does not mean that outdoors is 100% safe, and some cases of transmission (here and here) have been traced to outdoor conversations. Engaging in riskier activities outdoors may undo some of the benefits. Crowded outdoor locations, especially in more confined spaces (e.g. between two tall buildings) under low wind conditions and not in the sun, are the riskier ones. This is because there is less wind to disperse the virus-laden aerosols, and less UV to deactivate the virus.
The risk of transmission is much lower outside than inside because viruses that are released into the air can rapidly become diluted through the atmosphere. Again, think of the smoke analogy, if you are outdoors and you could inhale a lot of smoke if the people near you were smoking, then there is more risk. This virology professor at UMD thinks he was infected while waiting in line, while the wind was parallel to the line. Hard to prove, but plausible. But again, outdoors is much safer than indoors.
4.2. Does UV light from the sun kill the virus?
Yes, UV light from the sun is very effective at deactivating the virus, especially at high intensities, see the chart below. For example, the virus goes from surviving ~ 1 hr (at 21oC and 40% RH) to only 10 min. at a UV index of 2, and only ~2 min. Under intense full sun (UV index of 10).
Figure: decay rate of the viability of SARS-CoV-2 virus as a function of relative humidity and UV light. From DHS calculator |
This should be important for transmission through surfaces outdoors, as virus left on surfaces will be deactivated quickly during the day. It does not really matter for the aerosol or droplet pathways outdoors. Ballistic droplets will reach their targets (eyes, nostrils, mouth) in ~1 second, while if aerosols have not been inhaled in a few seconds, they will have diluted and moved away under typical outdoor winds of a few m/s.
4.3. Can I catch COVID-19 just by passing by someone indoors or outdoors?
It appears to take at least several minutes of exposure to the virus to become infected. While it is not impossible, there is no evidence that COVID-19 has been transmitted when people walk past each other outdoors. We recommend masks in shared indoor spaces at all times, and outdoors in crowded areas.
4.4. Is it safe to eat outdoors at a restaurant?
It is certainly safer to eat outdoors rather than indoors, but there should still be plenty of space between tables. If others are nearby, you should wear masks when not actively eating or drinking. Avoid tables that are directly downwind of occupied tables. When interacting with the server, you and the server should wear masks. People who do not live together should not share the same table, if the 2 m distance cannot be respected. SARS-CoV-2 transmit best when talking in close proximity, because aerosols (and ballistic droplets) are most concentrated there.
4.5. Is it safe to go to the swimming pool, beach, or park?
As long as it’s not crowded and people are able to maintain distance (and using masks when other people are closer) then recreating outdoors is a low-risk activity. The virus is not known to be transmitted through water.
5. Risk for specific situations
5.1. Is it safe to take a taxi cab or rideshare?
Being in a small, enclosed environment like the cab of a car can lead to high risk of infection if your driver (or customer if you are the driver) is infected with COVID-19. Your risk can be reduced significantly if you wear a mask and insist that the driver (or customer) wear a mask and you leave two windows at least partially open open during the trip. If the ventilation system is used, make sure it is set to outdoor air, and not to recirculated air (which would allow exhaled breath to accumulate). Since exposure time is important, shorter trips are better than longer trips. Try to avoid trips in a city during busy traffic times. Ventilation of the cab also increases with car speed, and so avoiding heavy traffic that leads to prolonged stops is safer, even when the windows are open.
5.2. Is it safe to travel by airplane?
Modern, large airplanes have very good ventilation and filtering. The risk during the flight is mainly from the people right next to you, which can be reduced by mask wearing and talking as little as possible. We recommend airlines that strictly enforce masking and leave the middle row empty. The boarding and unboarding process tend to have less ventilation, and thus mask wearing is especially important then.
Smaller airplanes used by regional airlines are less well characterized in terms of ventilation.
Often a significant fraction of the risk may be due to waiting inside the airport, taxi and bus rides, etc.
5.3 Are schools safe?
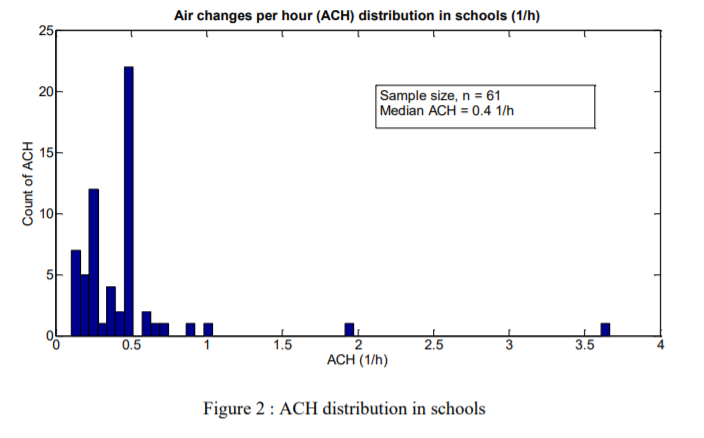
Unfortunately schools typically fulfill many the requirements for efficient virus transmission: indoors, crowding, low ventilation, close proximity, long duration, unmasked, talking/singing/yelling/breathing hard. Ventilation rates are often low, as shown in the figure below. There is a lot of debate about how well children transmit the disease, with some evidence that younger children transmit it less well, and older children transmit it as well as adults. But schools, if not modified, are also the perfect situation to transmit it, which may make up for lower inherent transmissibility. Per the precautionary principle, schools should only operate in person if the levels of infection in the community are low. It is imperative to implement several layers of protection, most importantly operating outdoors whenever possible. For class periods indoors, increased ventilation, masks, maintaining distancing, reducing the volume of speech, reducing density are all important. Monitoring CO2 levels and making sure that they stay below about 800-950 ppm is useful to make sure that the ventilation is sufficient. Joe Allen and collaborators at the Harvard School of Public Health have written extensively about this topic, and UC Berkeley has also published resources on this topic.
Figure: ventilation rates in air changes per hour (ACH) in multiple schools in California. (Source: Berkeley National Lab Report) |
5.4 What do you suggest for dental offices?
There is high aerosol generation in many dental procedures, which will aerosolize the saliva of the patient, which will contain the virus for infected people. Thus there is a risk for dental workers to be infected by the patient. The risk for the patient also exists, especially if the masks worn by the dental workers are not of sufficient quality or do not fit well.
The most important principle of indoor air quality is "source control." I.e. remove the contaminant where it is produced. “If there is a pile of manure in a space, do not try to remove the odor by ventilation. Remove the pile of manure.” Max von Pettenkofer, 1858).
In dentistry, source control takes the form of localized extraction of aerosols. It is the solution that makes the most sense by far. The air is extracted near the mouth of the patient, and either exhausted outside, or HEPA filtered. This type of thing (we don't endorse this particular one since we haven’t investigated it in detail). Localized extraction can be done provisionally quickly with limited cost.
Then use good masking, ventilation with outdoor air / filtering, and HEPA air cleaners, to mitigate against the aerosols that escape the localized extraction system. Localized extracting and these methods all work during the procedure when aerosols are highest and exposure is most important.
Also using an antiseptic (e.g. listerine) rinse can be useful for the patient, as they have been shown to be effective against viruses. However, the effect is thought to be short-lived, as only the viruses present in the saliva in that moment are deactivated. Quickly additional viruses will exit the cells and contaminate the saliva again (to our knowledge it has not been measured how quickly this happens). But if this was done every 10 min or so, it could help.
Foggers of bleach etc should be avoided. They can be dangerous if not enough time (> 30 min typically) is allowed for their chemicals to dissipate after application and before re-entering the room. And even if they killed all the viruses in the air, they are naturally less effective than the solutions above, because they work only after the procedure, not during the procedure when exposure time, virus concentration and thus risk are highest. Foggers should only be used for surface disinfection when nobody is present (although there may be easier ways to disinfect the surfaces).
5.5. What about elevators?
This Twitter thread and USEPA webinar (at about minute 52) by Prof. Richard Corsi (one of the writers of these FAQs) provides information on this issue. In short:
- Modern elevator cabins are generally well-ventilated with design air exchange rates as high as 1 per minute during travel plus additional air exchange when doors open at floors. These two factors indicate that there is relatively low risk of infection from breathing background air in an elevator cabin that might have previously transported an infector or even if you are in a cabin with an infector.
- That said, there are still many old elevators in use that are more like a closed box without ventilation. In this case the risk is much higher, and stronger precautions should be taken.
- The primary concern in elevators will be close contact (an infector breathing on you or speaking at you or others while facing you) and contaminated surfaces, e.g., floor buttons.
- Have as few people as possible at the same time in an elevator. A maximum of four allows a "corner per rider" (see below).
- Masks should be required of all elevator riders.
- No speaking should be allowed, as this significantly increases the number of aerosols (and ballistic droplets) released by an infector relative to breathing.
- Riders should avoid touching wall surfaces and should touch floor buttons with a disposable tissue, etc.
- Riders should sanitize hands after riding an elevator.
- If capable of doing so, it may be safer to take the stairs down. Going up, harder breathing can lead to higher emission of virus-laden aerosols and higher aerosol inhalation, which have to be weighed against the risk of sharing an elevator with others. For stairs that have very few people, taking the stairs should be better. If the stairs have several other people, then it is less clear. Masks should be worn while using stairs.
- Be careful about spending too much time in an elevator lobby on the ground floor of a building, where restrictions on number of passengers per car may result in high density and longer than normal duration of presence.
5.6. What about toilets?
SARS-CoV-2 is found in feces, but in almost all cases, it does not appear to be infectious. The virus has been found on toilet surfaces in patient rooms, but it is not clear whether it got there by contact or by deposition of aerosols. Virus can potentially spread via aerosols from toilets in two ways. First, flushing a toilet can generate aerosols: almost none for gravity-fed toilets used at home to millions for commercial flushometer toilets found in many public buildings in the US. The total volume of aerosols generated by a commercial toilet is low, comparable to the amount produced when a person says “Hello, world!” A study found two other types of viruses in the air in bathrooms in hospital and office buildings, but these were both respiratory viruses that could have come from people’s exhalations rather than flushing the toilet. A laboratory study of other types of viruses spiked into toilets was unable to detect them in the air after flushing. That said, it’s still a good idea to close the lid, if present, before flushing. Second, it is possible for fecal aerosols to spread through the plumbing system that connects units in a high-rise building, as occurred with the original SARS in the Amoy Gardens apartment buildings in Hong Kong, and several similar outbreaks in China and Hong Kong for COVID-19. In this case, the problem is bathroom floor drains (not common in the US) with dry traps that allow air from the vent stack, which might be contaminated with fecal aerosols from other units, to flow into your bathroom.
5.7. My specific situation is not here, what can I do?
You can submit a question in the feedback form, and we will add the most frequent ones as we have time to update these FAQs.
However there are so many situations that we can never address all of them there. The general pieces of advice are to think of the smoke analogy, and think about how much smoke people would breathe in your situation, if there was a smoker in the room. Also measuring CO2 in the space is a more sophisticated way to see how much exhaled air may be present in it. If you need to think about how the air is moving in your space, extinguish a mask or a candle in different points of the space, and see how the smoke moves.
6. Music
6.1. Are singing or playing wind instruments indoors dangerous?
Previous peer-reviewed studies have shown that singing generates aerosol. There are no peer-reviewed studies on wind instrument aerosol emissions. Numerous outbreaks have been reported of COVID-19 linked to large groups singing for long periods of time indoors with poor ventilation. There have been no reports of outbreaks due to wind instrument performances or rehearsals.
6.2. What kinds of instruments generate the most aerosol?
Studies are ongoing of emissions from singing, theater performances and wind and brass instruments at the University of Colorado Boulder and at University of Maryland. Based on preliminary measurements of aerosol emissions in the release flows while playing wind and brass instruments (mouth area, keyholes, end of instrument/bell) more aerosol is emitted from instruments that need significant back pressure to generate sound (e.g. oboe, clarinet, trumpet). Theater performing also generated more aerosol, compared to just talking.
6.3. What are the current recommendations to reduce aerosol emissions for musicians?
Recommendations include playing with masks with slits for mouth piece (can’t be done for certain instruments like oboe), wearing a mask while talking, playing with a bell cover, and practicing indoors for 30 min or less followed by a break for at least 1 air change (20 minutes at standard 3/hour) and possibly supplementing with a HEPA air cleaner to increase air changes (note an air cleaner is not a substitute for outdoor air ventilation).
6.4. What about playing music outdoors or using tents?
Playing music outdoors with social distancing and masks/bell covers is recommended. Tents without sides work like an indoor space with high ventilation rates and are fine.
6.5. What research is ongoing about transmission for choirs and wind instruments?
Please find information regarding the CU/Maryland COVID-19 Aerosol Study here: FAQs are on this page, with the ability to submit questions through a form on the website.
6.6. What do you think of the masks being sold for singers?
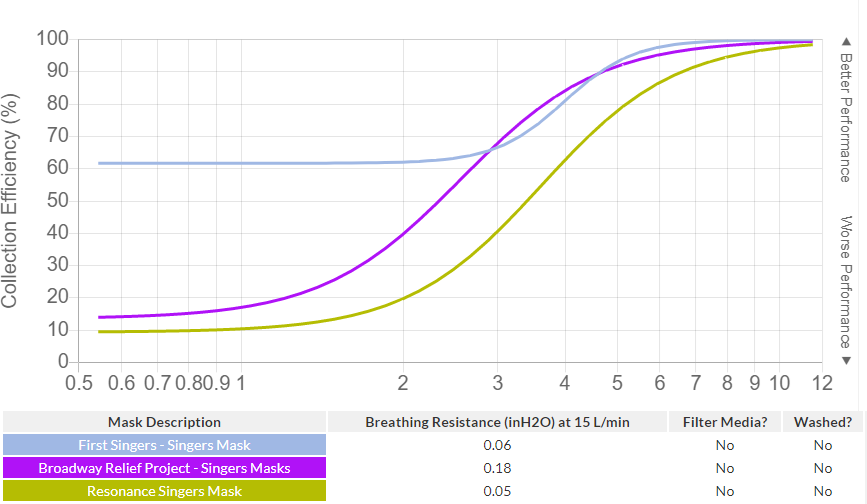
There are two important aspects: First, the fit of the mask to the face is key (not leaving gaps, nor developing gaps with strong breathing and singing). We have qualitatively tested two of the commercial singers’ masks and they seem fine in this regard. The second is the filtration characteristics of the masks. Prof. John Volckens at Colorado State Univ. has tested 3 commercial singers masks, see their database here. Results are reproduced below. This performance is not great, and there are far better masks available. Based on this we would only recommend these masks to sing outdoors. The manufacturers are making improvements so this may change in the future.
7. Masks and other protections
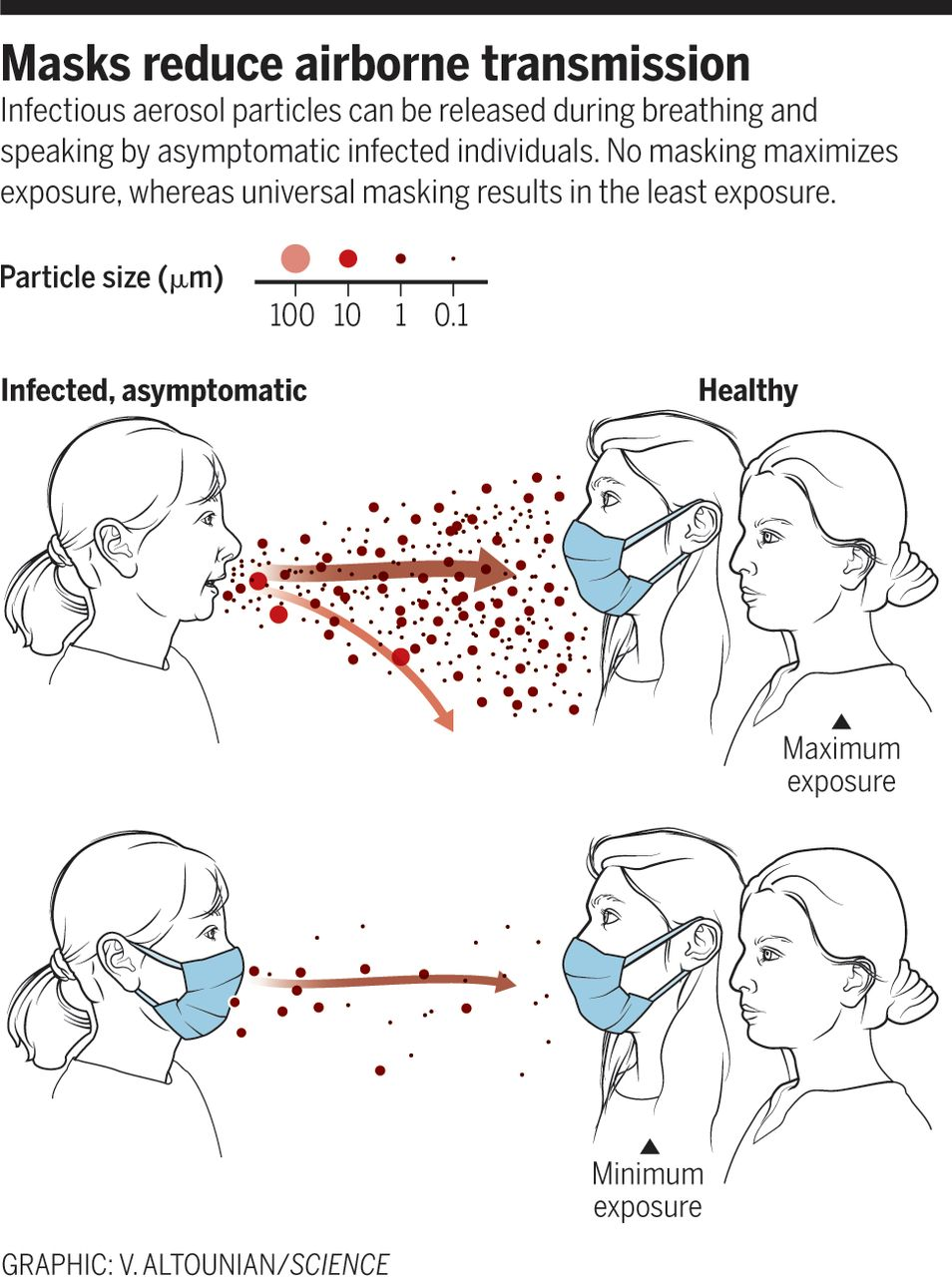
7.1. Do masks work to reduce the aerosol spread of COVID-19?
Yes! The physics are well understood. If a porous obstacle is put in the path of air that contains aerosols, some of the aerosols will end up in the obstacle. See the figure to the right from Science.
This video presents a good overview of filtration mechanisms of masks. The electrostatic mechanism discussed in the video is specific to N95 and surgical masks, but everything else is applicable to all masks.
Unfortunately there are many many misconceptions about masks, including:
- “Masks don’t work because the virus is much smaller than the pores of the mask.” First, the virus is not thought to be “naked” in the air, this is a misconception. Masks are just filters that we wear, so see this discussion below of filtering efficiency vs. size and why much of what you may hear online is wrong. Second, aerosol filtration does not work in the same way of a sieve that we may be more familiar with. Filters can capture aerosols that are much smaller than the pore size, see the Minute Physics video for a good explanation.
- “Masks do not work.” To say that masks do not work to remove a fraction of the aerosols (being either inhaled or exhaled) contradicts basic physics. It is like saying that if you put on a coat, you will not feel warmer. If you put on a coat, it will partially impede the flow of heat away from your body. In the same way a mask impedes the flow of particles across it, by capturing many of them. There is no other possibility. Of course the real efficiency depends on how good the mask material is as a filter, and of how well the mask fits without gaps.
- “Masks only protect against ballistic droplets, not aerosols.” Again, this is another misconception. Masks always provide some partial protection against exhaled and inhaled aerosols, with the protection depending on the quality of the mask material, how well they fit (no gaps between mask and face), and the size of the aerosols that matter.
- Some videos are circulating showing someone exhaling vaping aerosols, and concluding that masks don’t work based on that. This is wrong, as we discussed in this previous FAQ.
7.2. What is the best type of mask?
The effectiveness of a mask depends on two main factors: how well it fits and how well the material filters out aerosols of different sizes. A properly-fitted N95 respirator filters out at least 95% of aerosols of all sizes for the wearer. N95 respirators and other types of masks with valves allow aerosols to escape and do not protect others, so you should not use these; or if you do, put a piece of tape over the valve. The Chinese and South Korean versions of these, a KN95 and KF94, are excellent alternatives, although there are concerns about counterfeit KN95s that do not filter out aerosols well. Surgical masks are an excellent option, as they offer protection in the range of 70-80%, although there is wide variability among different brands. However, surgical masks tend to fit poorly, allowing aerosols to leak through gaps around the mask. A fitter, such as the Badger Seal, can greatly improve the effectiveness of a surgical mask. Cloth masks with pockets that can hold filters should be especially effective. Materials such as vacuum bags, HEPA filters, and MERV 13 filters perform well. Studies have found that homemade masks made out of tea cloth or cotton t-shirt material offer about 50% protection. Unpublished studies by Linsey Marr at Virginia Tech, John Volckens at Colorado State University, and Carl Wang at Missouri Science and Technology indicate that single layers of common fabrics have low filtration efficiencies for 0.3-μm aerosols but block about 50% of 2-μm aerosols and 80% or more of 5-μm and larger aerosols. If you use two layers or more of fabric, the overall efficiency can drastically increase to 90% or higher across all aerosol sizes larger than 0.5 μm. Virus is found in aerosols of all sizes, but those larger than 1 μm are probably most important for transmission. The mask should be worn covering the nose and mouth at all times when you are indoors with other people, except in your own residence or vehicle.
7.3. How effective are different types of masks for the wearer and for others?
See 7.2. What is the best type of mask? An N95 is expected to work well to protect others. A study showed that surgical masks can block 100% of seasonal coronaviruses (related to SARS-CoV-1) from spreading from an infected person into the air. Furthermore, unpublished results from Linsey Marr at Virginia Tech indicate that homemade masks, tested on a manikin, offer similar or slightly lower protection for the wearer (inward flow) than for others (outward flow).
7.4. Do I need to wear a mask outside?
When you regularly are passing by others at close distance (urban sidewalk) you should wear a mask outside. In situations where others are encountered outdoors infrequently it is good etiquette to either ensure adequate space between you and the other person, or wear a mask during the encounter.
7.5. Is it OK to just wear the mask over my mouth and leave my nose out?
No, the mask should cover your nose to block aerosols coming out of it and block any that you might breathe in from the air around you.
7.6. Is the fit of a mask important?
Yes, mask fit is crucial to protect against aerosols. If there are gaps, a substantial fraction of the air will flow through there. See examples in the figure below (stills from this great video). Some of the masks do not fit well, on purpose to illustrate what to avoid. The best fitting mask is the cloth mask on the right, and it shows the least leakage. If your mask fits well, you should feel the material suck up against your nose and mouth when you are breathing in. Many people wear poorly fitting masks, which significantly reduces their filtering efficiency. Perhaps this is partially left over from the initial introduction of masks to protect against ballistic droplets, which only need a “parapet” in between the two people, and where fit is much less important.
Figure: stills from mask visualization video showing leaks around gaps, which are major for the mask on the left, small for the mask in the middle, and not visible for the mask on the right.
7.7. Where should I stand around someone with a poorly fitting mask?
In this case you should avoid being behind and near the person. As the figure above shows, the curvature of the masks direct any exhaled aerosols in that direction.
7.8. Is it ok to remove my mask to talk?
No, unless you are outdoors at a sufficient distance. Speaking results in about x10 times more respiratory aerosol emission than just breathing, and singing (at high volume) or yelling can be about x50 times more. Ballistic droplets are not exhaled at all when breathing. You should also not allow others to talk to you without a mask from a close distance.
7.9. But I have seen some video online that shows vaping aerosols going through a mask. Doesn’t this show that masks don’t work?
In a word, no. Those videos make several errors and misconceptions, as discussed at the smoke FAQ above.
7.10. Are transparent masks safe?
It depends on the specific mask. The most important feature is that it must seal well around the face. If there are gaps, then it is not a useful mask. Then of course it has to filter aerosols well through the material through which the air will pass, and it should not fog, which are specific to each mask. Below are examples of masks that appear (from the pictures) to have gaps (left) or not (right). We haven’t tested these masks and do not endorse any in particular, just apply these principles to any transparent masks that you are considering.


Figure: examples of clear masks that appear to have visible gaps (left) vs not (right). We do not endorse any specific mask as we have not tested them, see text for criteria to identify potentially useful transparent masks.
7.11. Is there an easy way to assess my mask at home?
Several methods can be used:
- Inspect (or better, have someone inspect) the fit of the mask around your face. There should be no visible gaps. Make sure to test the mask under conditions similar to its use (e.g. talking, singing etc.).
- If the mask fits well, the air going through the mask cloth will push the mask closer to your face when inhaling, and away from your face when exhaling. This effect will vary with the tightness and material of the mask.
- Bill Nye the Science Guy suggests the candle test in this video starting at 1:30. This is a good indicator of how well a mask works, although it isn’t perfect.
- To test the fit over the bridge of your nose, John Volckens suggests standing in front of a mirror, exhaling quickly, and seeing if you blink. If you did not blink, then the seal around the top is probably good. If you did blink, then air is probably escaping around the bridge of your nose.
- Researchers at Georgia Tech suggest testing fabrics by their ability to block water droplets. All you need is a spray bottle and a mirror.
7.12. Do I need eye protection?
The eyes are thought to be a possible, but not major route of transmission for aerosols, because much more air is drawn into our lungs than may pass by our eyes. If someone was to cough or sneeze towards you, the risk from ballistic droplets impacting the eyes is significant. Some kind of eye protection can be useful to protect your eyes from ballistic droplets and aerosols, and also to keep you from sticking your fingers in your eyes. Some experts think this is useful, others think that it may be overkill, except in more crowded or risky environments. Regular glasses will be protective against ballistic droplets, while some kind of safety glasses that are more closed around the eyes, as in the figure below, is better for aerosols.
Figure: example of closed safety glasses to provide some protection against aerosol deposition on the eyes when needed. This particular model costs $8. |

7.13. Are face shields and masks interchangeable?
No, face shields do not offer much protection against aerosols (also see this video), while masks do. Face shields are good for blocking ballistic droplets released by the wearer or that might fly into the wearer's face when close to others. Face shields are considered a supplement to masks for partial eye protection (but less useful than closed glasses, as discussed above), but not a substitute for them.
7.14. Are plexiglass barriers helpful?
Plexiglass barriers are generally useful to avoid direct droplet infection and direct aerosol transmission whenever people are in close proximity and distance cannot be kept. Therefore, it is recommended to use them as a direct transmission suppression tool at such places, such as a supermarket checkout.
However, as aerosols follow the air movements indoors, the protective effects of the plexiglas barriers against aerosols will be limited. Plexiglas barriers alone are not a sufficient approach to protect against aerosol transmission. Their installation alone cannot protect against indoor aerosol transmission and should not be regarded as safe and sufficient protection. See the rest of these FAQs for more effective means of protection.
8. Ventilation
8.1. What do you mean by ventilation?
In this context ventilation means diluting indoor air with outdoor air. A fan that moves the air in the room is “mixing”, but not ventilation. Ventilation is useful because potentially virus-laden air indoors is diluted by virus-free air from outdoors, as shown in the schematic below. It is clear that superspreading tends to occur in low ventilation settings (e.g. this). This video shows some examples of the effect of different ventilation strategies on aerosol concentrations.
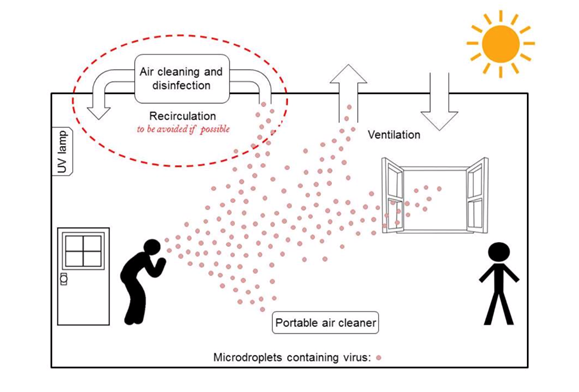
Figure: schematic of the effects of ventilation in removing virus-containing aerosols from indoor spaces. From Morawska et al. (2020).
8.2. Are windows a good way to increase ventilation?

Opening windows is the most basic method to increase ventilation, but the amount of ventilation through open windows can vary widely depending on the weather and other factors. Installing fans in windows to move more air (e.g. as in the picture) is preferred to ensure a more constant and continuous ventilation rate. Open other windows in the building so air is not sucked through cracks. Point any fans to blow out as you do not want to blow potential virus around the room.
However, open windows may not be practical when outdoor air is very hot or cold, or for locations without outside windows or with non-openable windows. In some buildings with mechanical ventilation systems (e.g. office buildings), opening the windows may be counterproductive, as it interferes with the ventilation system. In addition, outdoor air may not be “fresh”. Depending on location, outdoor air may contain allergens, fine aerosols, or trace chemicals. Air cleaners can help remove contaminants that enter through open windows
8.3. How are public buildings ventilated?
Mechanical ventilation systems operate in many public buildings, and supply and remove air through ducts. These systems vary hugely in their design and performance. Most can reduce aerosol concentrations via two methods. First, most systems can mechanically bring in outdoor air. The amount of air supply is determined by building codes and is mainly intended to control contaminants emitted by building materials and by occupants, not to control pathogens in the air. The ability to increase the flow of outdoor air above these minimum values is often limited by the ability to condition (control temperature and humidity) and distribute the air. For aerosol removal, filtration can supplement outdoor air ventilation if the proper filters are used. Filters rated MERV 13 and above can remove at least 80% of virus laden aerosols. However, not all air handling systems are designed to move air through these filters. Many do not have powerful enough fans and cannot be retrofitted with MERV 13 filters. Most building maintenance personnel can tell you what type of filter the building is using. This article in The Atlantic has an extensive discussion of this topic.
8.4. How can we quantify the ventilation rate in a space?
The ventilation rate is usually expressed in one of two ways:
- Air changes per hour (ACH). ACH refers to how quickly the air in a room is replaced with outdoor air, and does not take into account the number of people present. If ACH = 1 h-1, then after 1 h, 63% of the air has been replaced with outdoor air.
- Liters/second/person (L/s/p), which does take into account the number of people present, and is the most relevant parameter for preventing aerosol transmission of disease. The superspreading events that have been documented were in the range of 1-3 L/s/p. REHVA recommends at least 10 L/s/p, and if possible 20-25 L/s/p to mitigate COVID-19 transmission.
- The two quantities can be easily calculated from each other.
- L/s/p = V * (ACH/3600) / N, where V is the volume of the space in liters, and N is the number of occupants
ACH varies widely across different buildings:
- A study of schools in California found a median value of 0.4 ACH.
- Typical homes (with windows closed) range 0.5-1.5 ACH.
- Laboratories and older hospitals often have ~ 6 ACH.
- A new hospital in the US must meet 12 ACH in key areas
- There is wide variation from newer to older buildings, and across the world, and it is best to try to measure the ventilation rate for important spaces.
Determining ACH is a complex subject. Most building maintenance personnel won’t be able to tell you the current ventilation rate of a specific space, although they may be able to look up the designed value. Engineers and technicians who do testing and balancing and commissioning of systems can determine whether ventilation levels are correct. Because many HVAC systems are not well maintained, a current recommendation is that they be checked by professionals to determine whether they are functioning as designed and then updated as needed to enhance protections against COVID-19.
A good way to estimate the ventilation rate of a given space is to measure the decay rate of carbon dioxide (CO2) after an initial pulse with an affordable (~$150) meter as described in this post. This guide from Harvard discussed this topic in more detail. These methods require some familiarity with science and experiments. Do not confuse CO2 with carbon monoxide (CO), a highly toxic gas.
9. Monitoring ventilation using CO2 levels
9.1. Can we use the CO2 level in a space to estimate whether ventilation is good or bad?
Yes, this is a very useful technique, although it has some limitations. Outdoor CO2 is about 400 ppm, and human exhaled breath contains about 40000 ppm of CO2. Thus adding exhaled air to an indoor space rapidly increases the CO2 concentration. Since accurate, affordable CO2 meters are available, measuring CO2 is the best way to get a sense of the amount of exhaled air in a space. If you measure:
- ~400-500 ppm, the level of ventilation is very good
- ~800 ppm, 1% of the air you are breathing has already been breathed by someone in the space. This can start to be risky.
- ~4400 ppm, 10% of the air you are breathing has already been breathed by someone else. This is a very dangerous situation. Levels this high are commonly observed in densely occupied spaces with low ventilation such as many schools.
In well ventilated spaces, CO2 should stay below about 700 ppm to reduce COVID-19 infection risk. CO2 can be monitored with an affordable (~$150) meter as described below, which can be easily shared with many people.
The exact level considered “safer” for CO2 varies and we have seen various recommendations from 500 to 950 ppm. Choosing a general level like this is a compromise to make the method feasible and simple enough for many people. This is the same reason that a single distance (e.g. 1 m or 2 m) is quoted for social distancing (even though we know that 1.5 m is better than 1 m, and 2 is better than 1.5 m etc.). A key goal is to make clear that the many shared spaces with 2000 or 3000 ppm CO2 are unsafe, so that people realize that they have to take action to improve the situation there. Surveying classrooms, offices etc. with a CO2 monitor can be useful to determine which ones may have the worst ventilation, and prioritizing our actions there.
9.2. What are the limitations and caveats of the relationship between CO2 and infection risk?
There are several limitations and complexities that need to be taken into account when using CO2 as a surrogate of infection risk:
- In detail the relationship between the level of CO2 indoors and the risk of infection is complex, and depends on factors such as the number of people infected in a region, the amount of time spent in the indoor space, and the type of activity. For example activities such as singing or shouting, or strenuous exercise have a much higher risk for the same CO2 than sitting quietly, due to differences in the amount of aerosols exhaled and inhaled. For more details see this paper, or do some example calculations with the COVID-19 aerosol transmission estimator.
- Also air cleaning techniques such as filtration remove aerosols but do not change CO2. Thus in spaces where the air is filtered, a higher level of CO2 can be tolerated, although generally not beyond 1000 ppm due to other negative effects on humans. This calculator allows estimation of the tolerable CO2 levels for classrooms when filtering is also used.
- Another limitation for using CO2 as a tracer of exhaled breath arises if there are sources of CO2 such as cooking or space heating with fuels, with some of the combustion products staying in the space. Those sources must be turned off temporarily of their impact quantified for applying this technique. But in any case having combustion sources that vent the combustion air indoors is unsafe and should be rectified.
- A similar situation is measuring CO2 inside a car while in heavy urban traffic, or in an indoor space that is on a street with very busy traffic. In those cases outdoor CO2 in the street can be significantly higher than 400 ppm, let’s say 550 ppm. In those cases you have to add the extra outdoor CO2 to the limit, since that extra CO2 is not from human exhaled air. In this example the limit would go from 700 ppm to 850 ppm to account for this effect.
- Pets such as cats and dogs also exhale CO2, but this should be a small effect in most situations. Also domestic plants can take up and also emit CO2, but again the effect should be small.
9.3. How can we use continuous CO2 measurements to determine the right amount of natural ventilation in an indoor space?
For schools and other shared indoor spaces, the key is that the windows need to be open all the time while people are present at some level. This allows that any continuously-exhaled virus is constantly diluted and expelled outdoors, and not allowed to accumulate indoors. We do not recommend intermittent opening of the windows (e.g. 5 min. of every hour).
With the windows in a fixed position, and as long as the wind conditions don’t change, a "steady-state" is reached quickly. This means that the amount of exhaled CO2 is approximately equal to the amount of CO2 that leaves through the windows, so that the CO2 level in the room stays approximately constant. It is this approximately constant level that we need to keep below the desired target, e.g. 700 ppm. The graph below shows real data from a school in Spain. The bluish periods correspond to periods of transition, when people arrive or leave the room, or when something is changed with the ventilation (a window is open, in one of the 2 days shown).
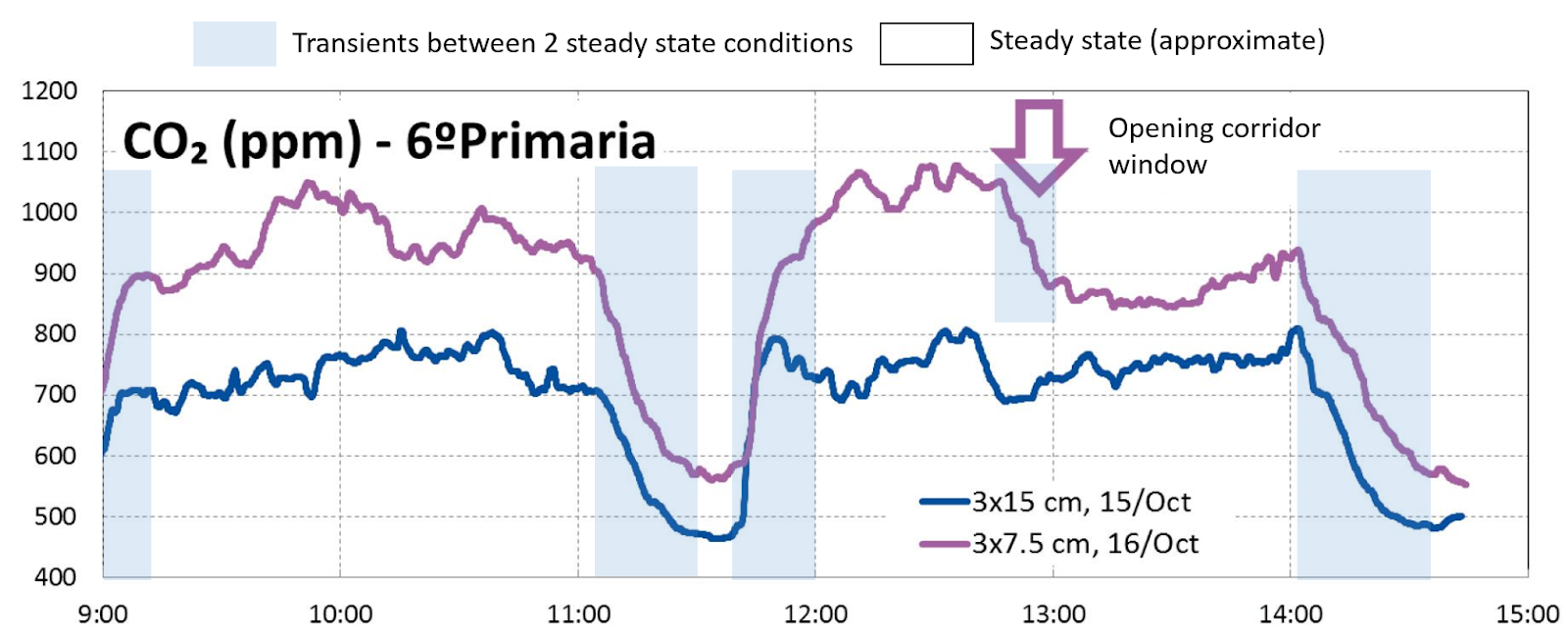
If the steady state CO2 is too high, then you have to open the windows a little more. If CO2 is lower than the limit and people are too cold/too hot, then you can close the windows a little. If you cannot find a way to keep CO2 low enough while keeping people thermally comfortable, then alternative actions are needed, e.g. air cleaning through filtration, reducing the number of people using the space, etc.
As shown in that example, opening 3 windows in a classroom only 15 cm was nearly sufficient to stay around 700 ppm. Thus typically it is not needed to keep all windows fully open. Importantly, the amount of window opening needed will depend on each particular building and room, and meteorological conditions (especially wind). Wind tends to increase the ventilation rate, and on windy days a similar CO2 level should be achievable with smaller window openings. A shared CO2 monitor (e.g. as a project for school students that visit different classrooms multiple times a day) can be used to quickly learn the amount of opening needed for a given indoor space as a function of wind conditions.
Ventilating corridors in schools (and other multi-room buildings) is very important, as otherwise they transfer exhaled air between classrooms.
9.4. What type of CO2 analyzers can be trusted?
We recommend NDIR (non-dispersive infrared) CO2 analyzers, which are typically priced in the $100-$200 range. Cheaper analyzers use other technologies that don’t really measure CO2, and their measurements are not trustworthy in our experience (e.g. they show very high CO2 values with it is very humid, when you use hand sanitizer next to them, and they don’t correlate well with higher-quality analyzers, etc.). The analyzer in the example below (Aranet4) was identified and tested by our REHVA colleagues and performed well against a research-grade analyzer, and in an intercomparison of several analyzers (we have no connection with that company). While this cost is too high for many individuals, the analyzers can be time-shared e.g. across a school, company, municipality, etc.
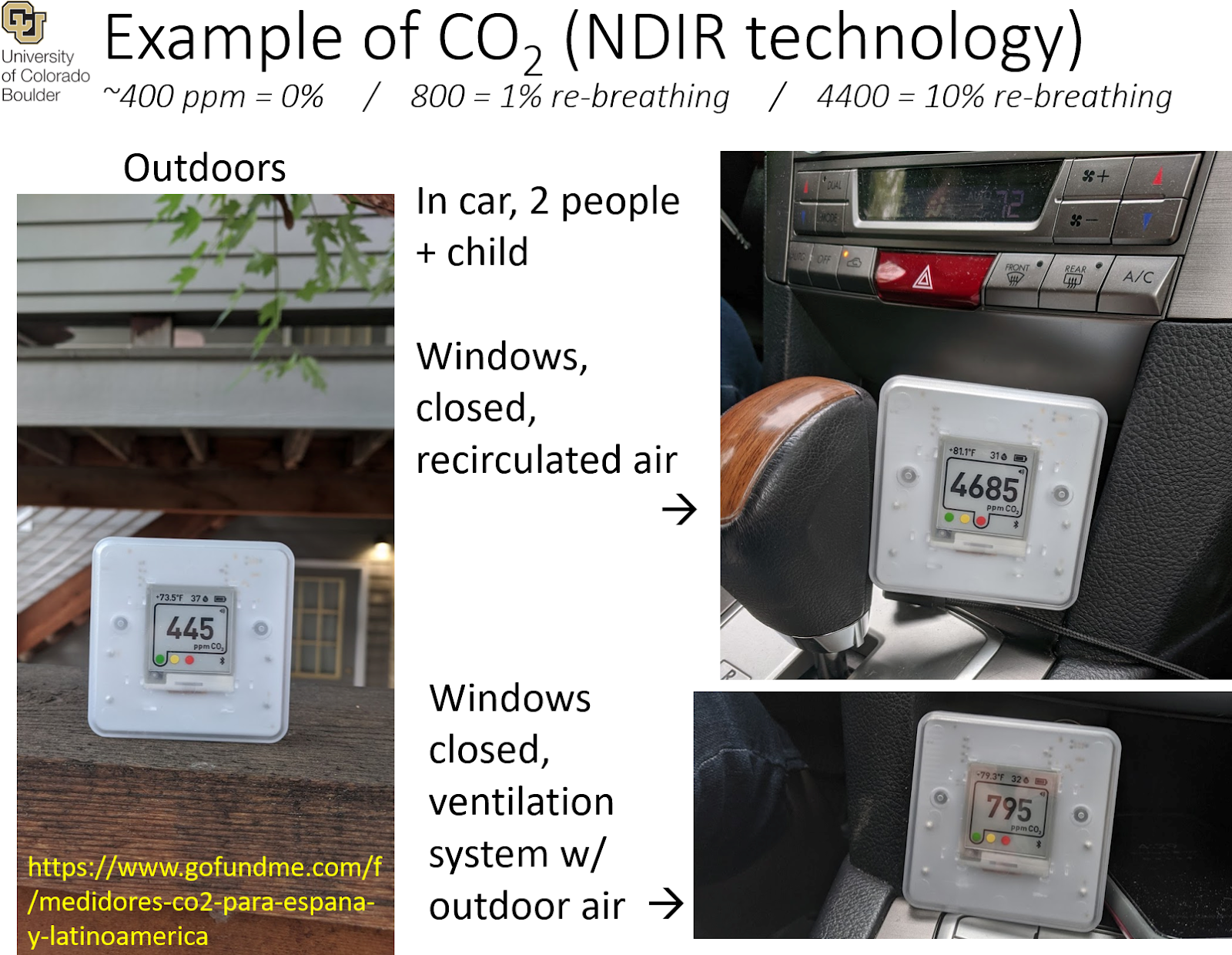
We are working with multiple colleagues to test other analyzers in the market, e.g. by comparing them with the Aranet4 or with research-grade analyzers, and we may recommend other models in the future. Also there are several initiatives trying to produce low-cost CO2 analyzers and make the designs available through open-sourcing. We support these efforts as well.
If you have test information on other analyzers that could be summarized or linked here (ideally scientific studies, but any well-done study from a reputable source is acceptable), please let us know. If other manufacturers are willing to provide analyzers for testing, let us know as well.
9.5. Where should I put the CO2 meter in a large room?
Ideally in the center of the room, around breathing height (1.5 m) or a little higher. Avoid placing it very close to people, as their direct exhaled breath (with ~40000 ppm CO2) could perturb the measurement. Also avoid placing them next to windows or HVAC supply vents where air is coming into the room. Placing them next to HVAC exhaust vents can be useful, since these sample the average air of the room.
You can also experiment by moving the CO2 meter to different locations in the room. Typically differences are small in most well-occupied rooms, once the steady state level has been reached.
9.6. Do you recommend measuring and displaying CO2 in all public places?
Yes, we recommend that going forward this becomes a standard measure of indoor air quality in all spaces where we breathe the same air as other humans. As this pandemic subsides, this would allow a more rational re-opening of indoor spaces, with limits on occupancy based on the amount of re-breathed air. This appears much preferable to arbitrary limits such as “restaurants can open at 50% capacity,” when we know that different restaurants may have very different degrees of ventilation.
After this pandemic subsides, there will be many other diseases of concern (including potential future pandemics) whose transmission can be reduced through ventilation. In addition there are other important chemical indoor air quality issues for which increased ventilation would also be useful. The figure below illustrates this proposal.

9.7. Can we instead measure the respiratory aerosols directly?
Yes, we can, but this can be more confusing. For CO2 human exhaled breath is a very strong source, and it normally dominates in indoor air. For aerosols, however, their number is typically dominated by infiltration of outdoor air aerosols, or by other indoor sources, such as cooking, smoking, or resuspension when walking.
For those who want to attempt this, you need a particle measurement device that reports data as a function of size. Respiratory aerosols are mostly > 1 micron, while most pollution, cooking, and smoking aerosols are smaller. However, resuspension when walking indoors also mostly produces aerosols > 1 micron. Thus walking should be avoided when trying to perform this measurement.
10. Filtering, and “air cleaning”
10.1. What filters should I use in my heating and/or air conditioning system?
Filters should efficiently remove particles in the size range of concern, especially those 10 μm or smaller, which includes most respiratory aerosol particles. All filters will help to reduce virus-containing aerosol concentrations, but standard filters have low efficiency in this size range and should be upgraded, if possible.
ASHRAE (the American Society of Heating, Refrigerating and Air-Conditioning Engineers) recommends, and the Centers for Disease Control (CDC) and others support, using at least MERV 13 filters as rated by ANSI/ASHRAE Standard 52.2. MERV stands for “Minimum Efficiency Reporting Value.” A comparable filter efficiency according to ISO Standard 16890 would be rated ePM1-50%. Both have high efficiency in the size range that contains most infections particles. A MERV 13 filter must remove at least 50% of particles between 0.3 and 1 μm, 85% from 1 – 3 μm and 90% from 3 – 10 μm.
Not all existing equipment is capable of handling MERV 13 filters due to the impact of higher pressure drop on system performance (i.e. the system fan may not be able to move enough air through a thicker filter than it was designed for). If this is the case, or if MERV 13 or higher filters are not available, the next highest rated available filter may be used. Existing systems should already have at least MERV 6 – 8 filters if designed to comply with codes based on ASHRAE Standards 62.1 and 62.2. Use of portable air cleaners with high efficiency - preferably HEPA - filters are another alternative if upgrade ability of existing filters is limited (see next question). ASHRAE’s COVID-19 guidance discusses how to evaluate how high a rating is feasible for a given system (see guidance on “Building Readiness”).
It is also very important to make sure filters are properly installed. They must fit tightly and not allow for any air – and particle - bypass through gaps between the filter and the filter holder. Leaks around the edges of the filter/filters will dramatically reduce their filtering efficiency.
10.2. Are portable air cleaners useful? Which types do you recommend?
Yes, portable air cleaners based on filtration are definitely useful. Our virus exposure risk is a function of aerosol concentration and time. For environments where we can’t reduce time, we can reduce the concentration. Portable air cleaners can effectively reduce indoor concentrations of virus relevant aerosol sizes.
Filtration does not have potential negative effects, and works very well to remove aerosols that may contain the virus. As a side benefit, allergies and pollution are also decreased, with additional health benefits.
Follow manufacturer guidelines for frequency of filter replacement. Unless the filter is being used in a space with high aerosol concentrations, in which case the filter should be replaced more often.
10.3. What are HEPA portable air cleaners?
“HEPA filter” is an acronym for “high efficiency particulate air filter.” They remove more than 99.9% of aerosols in an air stream passing through them. HEPA air cleaners are the best type of air cleaners (left picture below). They are simply a box with a fan that draws air through a high efficiency filter. The filter removes nearly all virus relevant aerosols. We recommend those without additional bells and whistles such as UV, ions etc. Those other features add cost and can add some problems. HEPA air cleaners need to be of the right size of the room, see this spreadsheet for helping to choose the right one. However they are costly, often in the hundreds of dollars or euros for a reasonably sized room.
Portable HEPA filter unit (Credit: Amazon) |
Improvised box-fan filtration unit (Credit: Jim Rosenthal) |

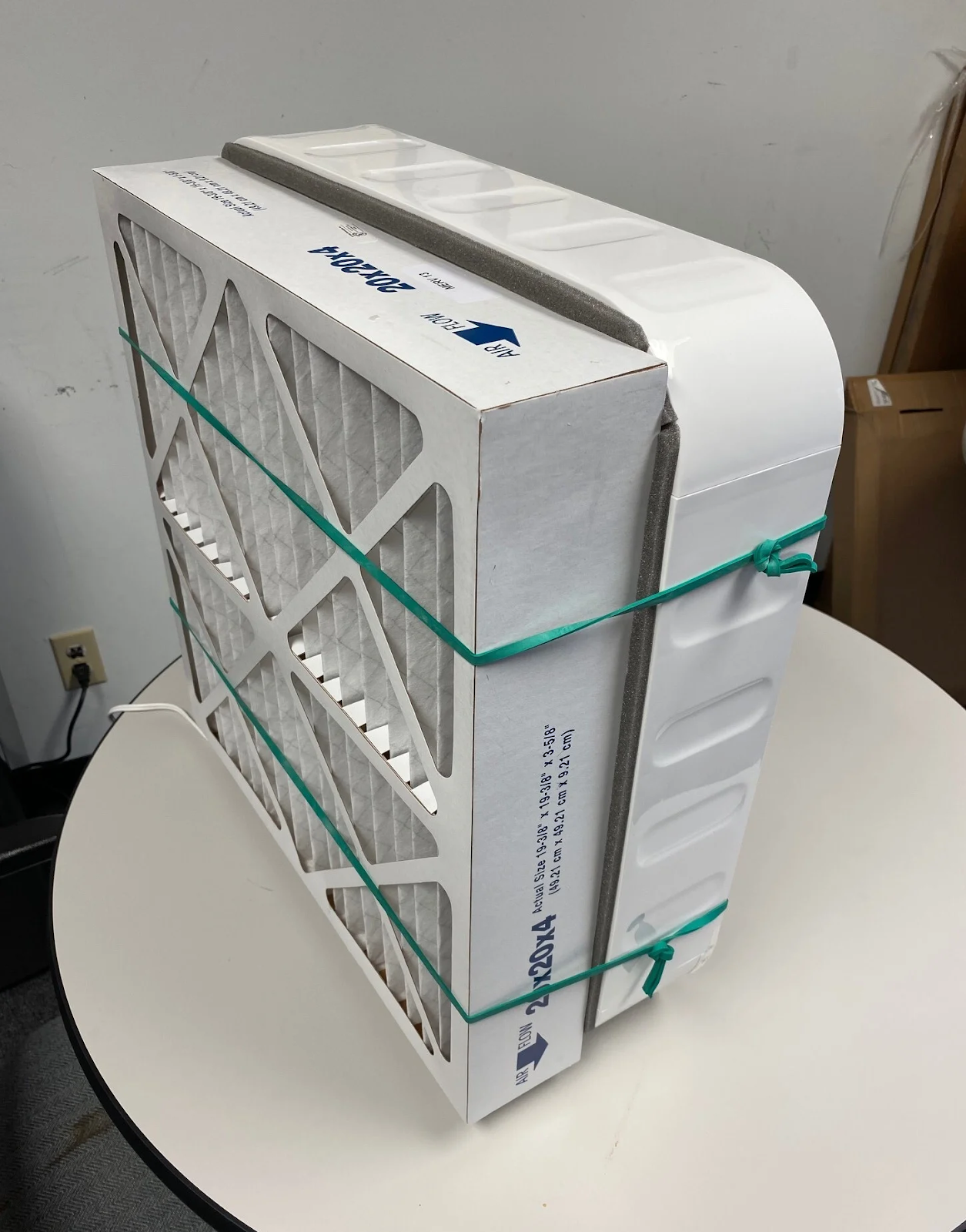
10.4. But if the virus is 0.1 μm, do HEPA / MERV filters (or masks) remove it from the air?
The virus is 0.1 μm (micrometers), but it is NOT naked in the air. The typical respiratory aerosol that contains viruses and is generated when talking is ~3 μm. See this question above.
And in any case all filters work well at 0.1 μm, because brownian motion helps a lot for filters to capture small aerosol . See the chart below from the American Society of Heating, Refrigeration, and Air Conditioning Engineers (ASHRAE) that shows the efficiency of the filtering mechanisms vs. aerosol size. There is a minimum at 0.3 μm because those aerosols are not well captured by either diffusion (which helps for the smaller ones) or impaction / interception (which helps for the larger ones). And filters and masks are often specified at 0.3 μm because that is the easiest measurement, since that is where most aerosols penetrate the filter. Also 0.3 μm is a typical size for pollution and smoke aerosols, but NOT for virus-containing respiratory aerosols, which are mostly larger. This video discusses the subject very clearly.
Figure: efficiency of different physical mechanisms of filtering vs. aerosol size (source). |
Figure: efficiency vs different MERV13 filter grades and of HEPA filters (nearly 100% at all sizes) vs. aerosol size (from ASHRAE) |
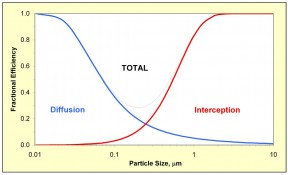
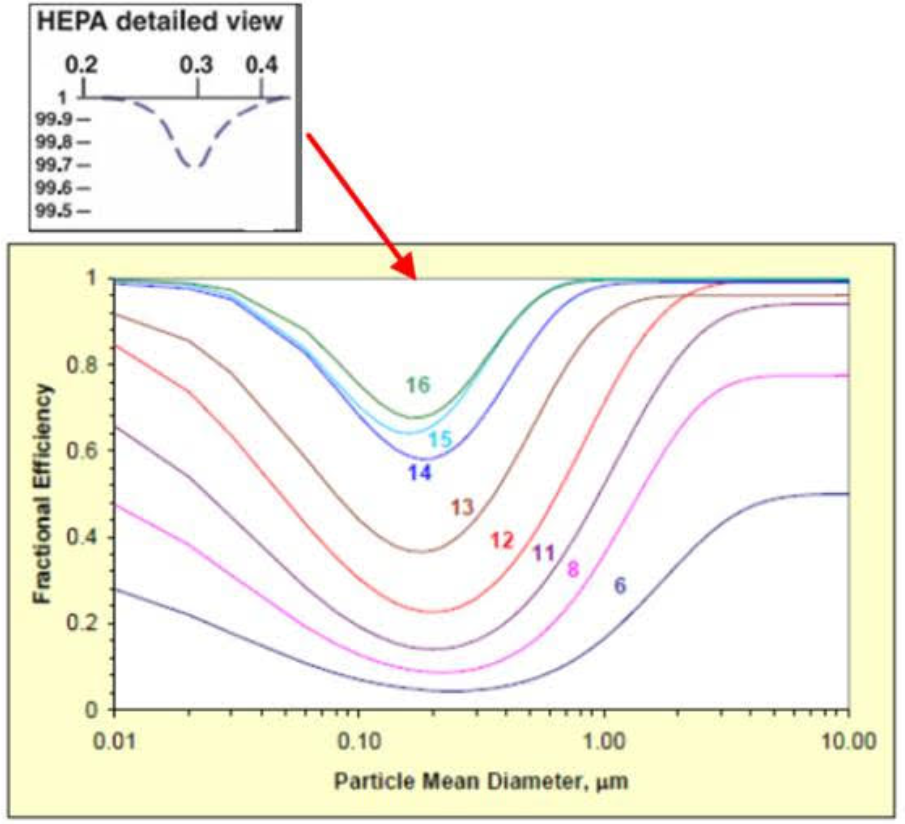
10.5. Is there a cheaper alternative to a HEPA air cleaner?
Yes, a makeshift fan-filter system (right picture above) often costs one fifth as much as a portable HEPA unit, and can be very effective at removing aerosols from a room. This article in Wired and this first and second articles from the CEO of a filter company discuss the idea of do-it-yourself systems. These may be noisier as well. Some tips for these:
- You should close the gaps between the filter and the fan with tape to remove leaks
- Use a deeper filter, which allows more airflow and a more efficient filtering
- MERV 13 or similar is recommended. A HEPA filter may cause too high pressure drop, causing the fan to work too hard. The fan then may overheat and/or fail prematurely. Only operate this system when someone is present to monitor the system.
- From the point of view of filtering, it is better to put the filter in the intake side (where the fan is pulling air from). But then any virus is exposed to the touch. So e.g. in a classroom it may be better to put the filter on the exhaust side, so that any virus is not exposed (but then taping it around the fan is even more important)
- With most fans the system will work better at a lower setting. The full speed setting may lead to too much force on the filter, and overheating of the fan. A lower setting will also reduce noise. The details will depend on the fan / filter combination. If there is too much noise or overheating of the fan, consider a lower filter grade.
- Monitor the temperature of the fan, and don’t leave the system operating unattended. There could be some risk of fire if the fan motor overheated for a prolonged period of time.
- See below about how to change the filter.
10.6. How do I select the right HEPA air cleaner? (or fan-filter cleaner)
There are products of various quality in the market. Some work well, others have lower quality filters that may not seal so well etc. We cannot give advice on specific models. We suggest that you select ones:
- with just the filter (if possible, so no ions, UV etc.)
- that are recommended by certifying authorities (AHAM or CARB in the US, Eurovent in Spain).
- that you consult also the Harvard-Univ. of Colorado guide.
- It is important that the size is large enough for the space. Any amount of filtering will help. To see the effect on the probability of infection for a specific situation, you can use the Aerosol Transmission Estimator (more advanced). The Harvard School of Public Health recommends 5 air changes per hour (ACH) for schools. To calculate this number, you can use the calculator in the Harvard-Univ. of Colorado guide, or simply calculate as in this example:
- Volume of the room = 5 m x 3 m x 3 m = 45 m3
- Clean air delivery rate (CADR) of the HEPA unit = 200 m3 / hr
- ACH = 200/45 = 4.4 h-1 (which is pretty close to 5)
- If you use more than one unit, then sum the ACH
- Note that the CADR of the unit can vary with the setting (e.g. low / high speed)
- For cheap fan-filter combinations, estimating the CADR is a little trickier. The manual of the fan (which can often be found at the manufacturer’s website) should have a specification of flow rate (m3/h or similar units) for each setting. Then the filter will reduce the flow rate. We suggest taking 60% of the nominal flow rate without the filter as the CADR in the calculation above.
10.7. Where should I place a HEPA air cleaner in a room?
In general most commercial portable air cleaners draw air in from the side and exhaust it vertically. For these systems, place the portable air cleaner in the middle of the room, raised off the floor if possible. This placement is to make sure as much of the room air gets to the filter as possible. If the air cleaner is placed near a wall, air on one side of the room will be filtered faster than the other side. Ensure the cord is secure so no tripping hazard exists.
For DIY systems, elevation may be more important due to the typical horizontal exhaust. A strong airflow over the floor may resuspend aerosols that have settled. A vertical exhaust is also desirable, and can be done.
10.8. How and when should filters be replaced?
When filters collect lots of aerosols, the airflow through the filter generally goes down and the pressure drop across the filter increases (pressure on one side minus pressure on the other side). When the pressure increases it becomes harder and harder for the blower to pull air through the filter. This can result in lower air flow rates, overheating and damage to the blower, etc. To maintain the effectiveness of the filter in cleaning room air replace the filters according to manufacturer's guidelines. Typically this is six months to a year for HEPA filters and three to six months for pre-filters. In dirty environments (spaces with high aerosol concentrations such as where there are smokers or dust) replacement may need to occur more frequently.
Wear a mask and gloves when removing filters, and change the filter outdoors if possible. These recommendations are because physically manipulating a filter that may have just collected virus-containing aerosols can cause the aerosols to dislodge and be resuspended in the air. Place the used filters in a sealed plastic bag prior to disposal. Any viruses that have been removed from the air will be in the filter. It is possible that they die within a few hours, as they do in aerosols, or within a few days, as they do on surfaces (to our knowledge this has not been studied). It is not easy to get any viruses trapped in the filter back into the air, but it is possible in principle. So if the filter has been used within a few days in a location where there could be viruses, then just out of an abundance of caution follow the above precautions. And if possible, change the filter after it has not been used for a few days. e.g. in an office or classroom, you could change it first thing on Monday morning, before work or classes start. Again, we think this is a (very) small risk, but better to be safe just in case.
10.9. Is germicidal ultraviolet light (UVC) effective as an air disinfection treatment for SARS-CoV-2?
Germicidal ultraviolet light (gUV, also UVC) is an effective technology to use to supplement ventilation. It is especially useful for increasing effective air change rates in spaces that are heavily occupied, and have the potential for unsuspected infectious persons inside. Data is forthcoming on the inactivation rates specifically for CoV-2 but in the meantime comparing rates for coronaviruses it appears to be as susceptible to gUV as the organism that causes tuberculosis is (Mycobacteria tb.).
One application that has been used since the early part of the 1900s is upper-room gUV. Lamp fixtures are hung higher up the walls to irradiate the upper part of the room only. The lamp fixtures have louvers that direct the UV radiation across the room. Studies in the laboratory have shown that these systems can add as much as 17 air changes per hour. This type of system was used in NY classrooms to combat measles and was installed in many facilities during the resurgence of tuberculosis in the late 1990s. The CDC has authored a guideline for the use of upper-room gUV in healthcare. Germicidal UV can also be applied in ducts of the recirculating air in an HVAC system. This design must consider the velocity of the air passing through the UV to allow for sufficient contact time. It is also recommended to install these in the mixed air plenum, as performance is improved.
New technology at 222 nm is being developed and commercialized. It has a major advantage vs. the traditional 254 nm technology, in that it can be shone directly on people, because it does not penetrate the skin. It is still expensive and not widely available.
Dr. Shelly Miller has been studying gUV for over 20 years and here is a link to slides from a presentation she gave in April 2020. For a summary and additional citations, see section 2.4 of the following paper that was published by some of the authors of this FAQ: How can airborne transmission of COVID-19 indoors be minimised?
10.10. Do you recommend portable air cleaners that are not based on filtration?
We do not recommend other types of air cleaners (ions, plasmas, oxidation etc.) for general purpose use, see this thread for more details.
10.11. Do you recommend spraying disinfectants into indoor air to kill the virus?
Definitely not for cleaning the virus in the air. This technique can be useful for disinfecting surfaces, when nobody will be present in the space for at least three air change rate timescales. If you don’t know the air change timescale for the space assume that you need at least 3 hours. See this Twitter thread and the same info as a Medium post for more details on the issues for some of these systems.
10.12. Should we use humidifiers or dehumidifiers?
It is well-known that dry conditions favor the survival of SARS-CoV-2 and similar viruses. This only matters for transmission at a distance; transmission in close proximity is not impacted by humidity or temperature. In principle humidifiers can be used to increase humidity and reduce the survival time of the virus. However, ventilation and/or filtering of indoor air is much simpler and more efficient. Ventilation expels the virus-containing aerosols outdoors, while filtering captures them and removes them from the air we breathe. Humidifying alone does not physically remove the virus from the air, but it may make the virus decay faster.
Dry conditions may also make humans more susceptible to infection, which would suggest that humidification to avoid dry conditions can be beneficial.
Given its simplicity and efficacy in removing the virus from the air, we recommend that any investment is focused on ventilation and filtering (and potentially germicidal UV, when professionals can do it). We recommend humidification for people who already own humidifiers and want to add an additional layer of protection. REHVA’s guidance agrees with this point. The relative humidity should remain below 65% to avoid promoting mold growth.
Dehumidifiers are often used in locations where humidity is very high, to prevent mold growth and reduce associated odors. However, we advise against using them if the relative humidity is below 40% because they could make the air too dry.
10.13. Should we keep indoor spaces hotter or colder to reduce transmission?
Viruses survive less well at higher temperatures. However, higher temperatures reduce relative humidity, and low humidity leads to increased survival of the virus. Both effects are relatively small over a few degrees of change under typical comfortable ranges. Therefore at present we do not recommend changing ambient indoor temperatures for this purpose. REHVA’s guidance agrees with this point.