
Adding Walnuts to the Usual Diet Can Improve Diet Quality in the United States: Diet Modeling Study Based on NHANES 2015–2018

Abstract
:1. Introduction
2. Materials and Methods
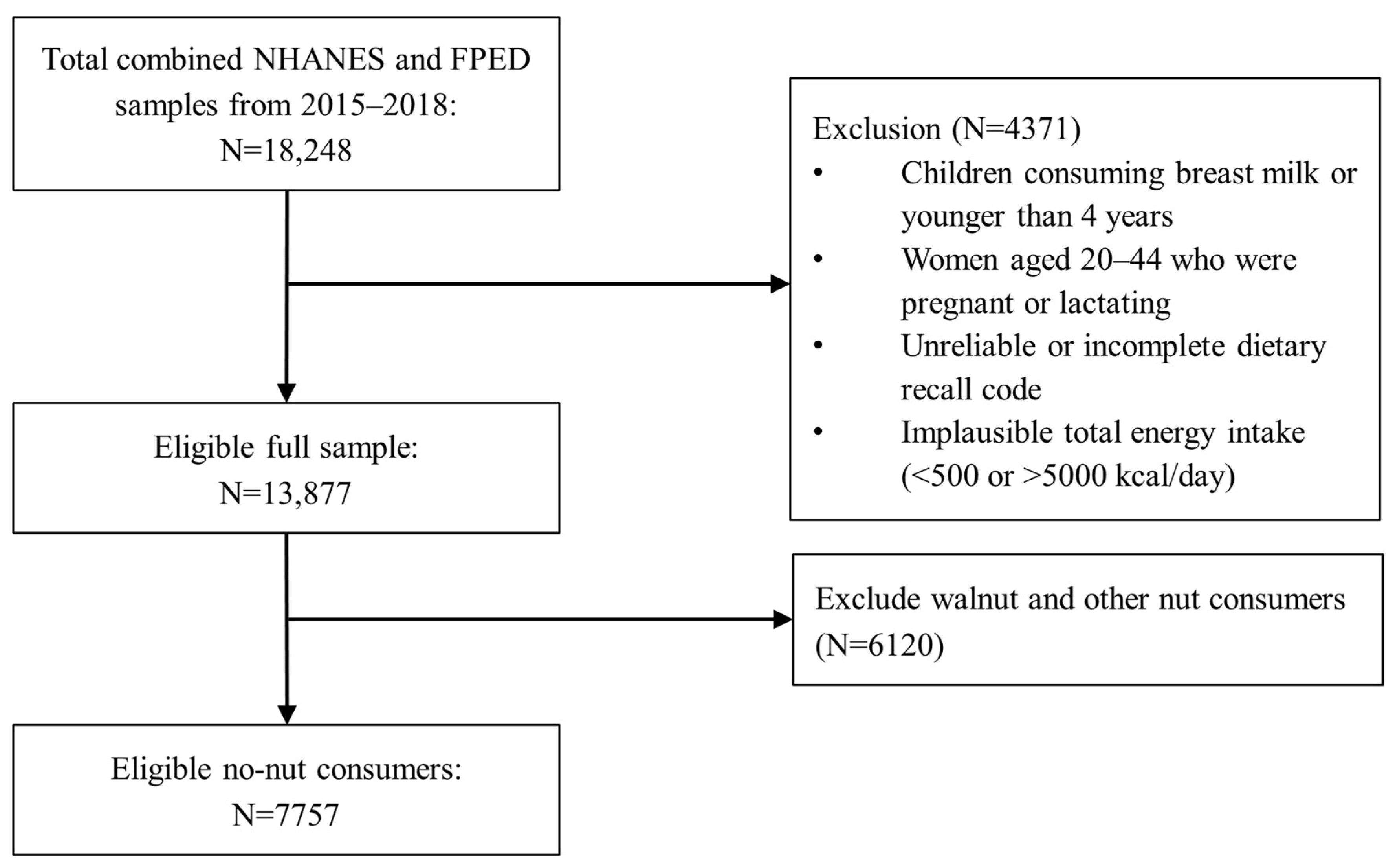
2.1. Study Population
2.2. Dietary Intake Measures
2.3. Food Composition Data
2.4. Walnut Consumption Classification
2.5. Modeling
2.6. Analyses
3. Results
3.1. Demographics and Walnut Consumption
3.2. Impact of Walnut Consumption on Nutrient Adequacy
3.2.1. Magnesium
3.2.2. Folate
3.2.3. Potassium
3.2.4. Fiber
3.2.5. Other Vitamins, Minerals, and Omega-3 Fatty Acids
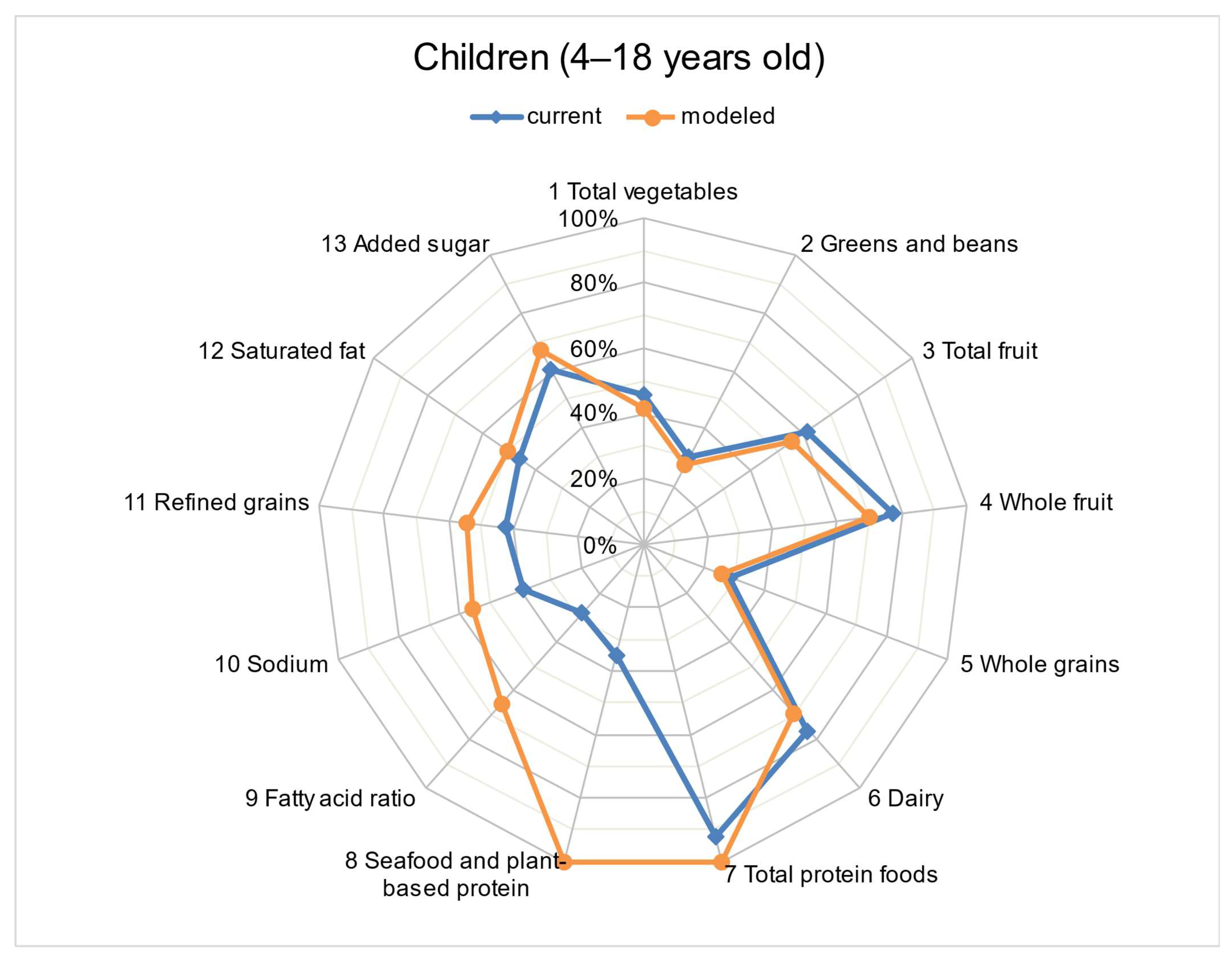
3.3. Diet Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025, 9th ed.; U.S. Department of Agriculture and U.S. Department of Health and Human Services: Washington, DC, USA, 2020. Available online: DietaryGuidelines.gov (accessed on 10 November 2021).
- Ros, E.; Hu, F.B. Consumption of plant seeds and cardiovascular health: Epidemiological and clinical trial evidence. Circulation 2013, 128, 553–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.; Tsao, R.; Yang, R.; Kramer, A.J.K.G.; Hernandez, M. Fatty Acid Profiles, Tocopherol Contents, and Antioxidant Activities of Heartnut (Juglans ailanthifolia Var. cordiformis) and Persian Walnut (Juglans regia L.). J. Agric. Food Chem. 2007, 55, 1164–1169. [Google Scholar] [CrossRef] [PubMed]
- California Walnut Board. California Walnuts: A Guide to Serving Walnuts in Schools; California Walnut Board: Sacramento, CA, USA, 2018. [Google Scholar]
- Hayes, D.; Angove, M.J.; Tucci, J.; Dennis, C. Walnuts (Juglans regia) chemical composition and research in human health. Crit. Rev. Food Sci. Nutr. 2016, 56, 1231–1241. [Google Scholar] [CrossRef]
- Ros, E. Nuts and CVD. Br. J. Nutr. 2015, 113 (Suppl. 2), S111–S120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajaram, S. Health benefits of plant-derived α-linolenic acid. Am. J. Clin. Nutr. 2014, 100 (Suppl. 1), 443S–448S. [Google Scholar] [CrossRef] [Green Version]
- Banel, D.K.; Hu, F.B. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: A meta-analsis and systematic review. Am. J. Clin. Nutr. 2009, 90, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Li, J.; Hu, F.B.; Salas-Salvadó, J.; Tobias, D.K. Effects of walnut consumption on blood lipids and other cardiovascular risk factors: An updated meta-analysis and systematic review of controlled trials. Am. J. Clin. Nutr. 2018, 108, 174–187. [Google Scholar] [CrossRef] [Green Version]
- García-Conesa, M.T.; Chambers, K.; Combet, E.; Pinto, P.; Garcia-Aloy, M.; Andres-Lacueva, C.; De Pascual-Teresa, S.; Mena, P.; Ristic, A.K.; Hollands, W.J.; et al. Meta-analysis of the effects of food and derived products containing ellagitannins and anthocyanins on cardiometabolic biomarkers: Analysis of factors influencing variability of the individual responses. Int. J. Mol. Sci. 2018, 19, 694. [Google Scholar] [CrossRef] [Green Version]
- Ros, E.; Izquierdo-Pulido, M.; Sala-Vila, A. Beneficial effects of walnut consumption on human health: Role of micronutrients. Curr. Opin. Clin. Nutr. Metabl. Care 2018, 21, 498–504. [Google Scholar] [CrossRef]
- Corwin, R.L.; Hartman, T.J.; Maczuga, S.A.; Graubard, B.I. Dietary saturated fat intake is inversely associated with bone density in humans: Analysis of NHANES III. J. Nutr. 2006, 136, 159–165. [Google Scholar] [CrossRef]
- Hu, F.B.; Willett, W.C. Optimal diets for prevention of coronary heart disease. J. Am. Med. Assoc. 2002, 288, 2569–2578. [Google Scholar] [CrossRef] [PubMed]
- King, J.C.; Blumberg, J.; Ingwersen, L.; Jenab, M.; Tucker, K.L. Tree nuts and peanuts as components of a healthy diet. J. Nutr. 2008, 138, 1736S–1740S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health and Nutrition Examination Survey (NHANES). MEC In-person Dietary Interviewers Procedural Manual. 2017. Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/manuals/2017_MEC_In-Person_Dietary_Interviewers_Manual.pdf (accessed on 10 November 2021).
- U.S. Department of Agriculture, Agricultural Research Service. USDA Food and Nutrient Database for Dietary Studies 2015–2016. Food Surveys Research Group Home Page. 2018. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 10 November 2021).
- U.S. Department of Agriculture, Agricultural Research Service. USDA Food and Nutrient Database for Dietary Studies 2017–2018. Food Surveys Research Group Home Page. 2020. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 10 November 2021).
- Bowman, S.A.; Clemens, J.C.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2017–2018, Methodology and User Guide. Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service, U.S. Department of Agriculture, Beltsville, MD, USA. 2020. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 10 November 2021).
- Bowman, S.A.; Clemens, J.C.; Shimizu, M.; Friday, J.E.; Moshfegh, A.J. Food Patterns Equivalents Database 2015–2016, Methodology and User Guide; Food Surveys Research Group, Beltsville Human Nutrition Research Center, Agricultural Research Service; U.S. Department of Agriculture: Beltsville, MD, USA, 2018. Available online: http://www.ars.usda.gov/nea/bhnrc/fsrg (accessed on 10 November 2021).
- U.S. Department of Agriculture, Agricultural Research Service. FoodData Central; 2019. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-details/170187/nutrients (accessed on 10 November 2021).
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. Dietary Guidelines for Americans 2015–2020, 8th ed.; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, 2015.
- Tooze, J.A.; Kipnis, V.; Buckman, D.W.; Carroll, R.J.; Freedman, L.S.; Guenther, P.M.; Krebs-Smith, S.M.; Subar, A.F.; Dodd, K.W. A mixed-effects model approach for estimating the distribution of usual intake of nutrients: The NCI method. Stat Med. 2010, 30, 2857–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usual Dietary Intakes: SAS Macros for Analysis of a Single Dietary Component 18 February 2015. Available online: https://epi.grants.cancer.gov/diet/usualintakes/macros.html (accessed on 14 August 2021).
- National Cancer Institute. Usual dietary intakes: SAS macros for analysis of a single dietary component. Available online: https://epi.grants.cancer.gov/diet/usualintakes/macros_single.html (accessed on 10 November 2021).
- Institute of Medicine (US) Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes: Applications in Dietary Planning; National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- National Cancer Institute. The Healthy Eating Index—Population Ratio Method. Available online: https://epi.grants.cancer.gov/hei/population-ratio-method.html (accessed on 10 November 2021).
- Arab, L.; Guo, R.; Elashoff, D. Lower Depression Scores among Walnut Consumers in NHANES. Nutrients 2019, 11, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njike, V.Y.; Ayettey, R.; Petraro, P.; Treu, J.A.; Katz, D.L. Walnut ingestion in adults at risk for diabetes: Effects on body composition, diet quality, and cardiac risk measures. BMJ Open Diabetes Res. Care 2015, 3, e000115. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. PREDIMED Study Investigators. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [Green Version]
- Akbaraly, T.N.; E Ferrie, J.; Berr, C.; Brunner, E.; Head, J.; Marmot, M.; Singh-Manoux, A.; Ritchie, K.; Shipley, M.J.; Kivimaki, M. Alternative Healthy Eating Index and mortality over 18 y of follow-up: Results from the Whitehall II cohort. Am. J. Clin. Nutr. 2011, 94, 247–253. [Google Scholar] [CrossRef] [Green Version]
- Atkins, J.L.; Whincup, P.; Morris, R.; Lennon, L.; Papacosta, O.; Wannamethee, S. High diet quality is associated with a lower risk of cardiovascular disease and all-cause mortality in older men. J. Nutr. 2014, 144, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef]
- Rehm, C.D.; Drewnowski, A. Replacing American snacks with tree nuts increases consumption of key nutrients among US children and adults: Results of an NHANES modeling study. Nutr. J. 2017, 16, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neil, C.E.; Keast, D.R.; Nicklas, T.A.; Fulgoni, V.L., 3rd. Out-of-hand nut consumption is associated with improved nutrient intake and health risk markers in US children and adults: National Health and Nutrition Examination Survey 1999–2004. Nutr. Res. 2012, 32, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Tey, S.L.; Brown, R.; Gray, A.; Chisholm, A.; Delahunty, C. Nuts assist with weight maintenance while improving diet quality. Ann. Nutr. Metab. 2011, 58 (Suppl. 3), 12. [Google Scholar] [CrossRef] [Green Version]
- Bitok, E.; Rajaram, S.; Jaceldo-Siegl, K.; Oda, K.; Sala-Vila, A.; Serra-Mir, M.; Ros, E.; Sabaté, J. Effects of Long-Term Walnut Supplementation on Body Weight in Free-Living Elderly: Results of a Randomized Controlled Trial. Nutrients 2018, 10, 1317. [Google Scholar] [CrossRef] [Green Version]
- Uwitonze, A.M.; Razzaque, M.S. Role of Magnesium in Vitamin D Activation and Function. J. Osteopath. Med. 2018, 118, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Maier, J.A.; Castiglioni, S.; Locatelli, L.; Zocchi, M.; Mazur, A. Magnesium and inflammation: Advances and perspectives. Semin. Cell Dev. Biol. 2021, 115, 37–44. [Google Scholar] [CrossRef]
- US Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 28. Available online: https://ndb.nal.usda.gov/ndb/ (accessed on 20 November 2021).
- Green, R.; Datta Mitra, A. Megaloblastic Anemias: Nutritional and Other Causes. Med. Clin. N. Am. 2017, 101, 297–317. [Google Scholar] [CrossRef]
- Osredkar, J.; Sustar, N. Copper and Zinc, Biological Role and Significance of Copper/Zinc Imbalance. J. Clin. Toxicol. 2011, S3, 495. [Google Scholar] [CrossRef] [Green Version]
- Roohani, N.; Hurrell, R.; Kelishadi, R.; Schulin, R. Zinc and its importance for human health: An integrative review. J. Res. Med. Sci. 2013, 18, 144–157. [Google Scholar]
- Kris-Etherton, P.M.; Taylor, D.S.; Yu-Poth, S.; Huth, P.; Moriarty, K.; Fishell, V.; Hargrove, R.L.; Zhao, G.; Etherton, T.D. Polyunsaturated fatty acids in the food chain in the United States. Am. J. Clin. Nutr. 2000, 71 (Suppl. 1), 179S–188S. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Y.; Huang, W.; Peng, C.; Zhang, J.; Wong, C.; Kim, J.H.; Yeoh, E.K.; Su, X. Effect of nut consumption on vascular endothelial function: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2018, 37, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Blondeau, N.; Lipsky, R.H.; Bourourou, M.; Duncan, M.W.; Gorelick, P.B.; Marini, A.M. Alpha-linolenic acid: An omega-3 fatty acid with neuroprotective properties-ready for use in the stroke clinic? Biomed. Res. Int. 2015, 2015, 519830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathur, P.; Ding, Z.; Saldeen, T.; Mehta, J.L. Tocopherols in the prevention and treatment of atherosclerosis and related cardiovascular disease. Clin. Cardiol. 2015, 38, 570–576. [Google Scholar] [CrossRef]
- Abdallah, I.B.; Tlili, N.; Martinez-Force, E.; Rubio, A.G.P.; Perez-Camino, M.C.; Albouchi, A.; Boukhchina, S. Content of carotenoids, tocopherols, sterols, triterpenic and aliphatic alcohols, and volatile compounds in six walnuts (Juglans regia L.) varieties. Food Chem. 2015, 173, 972–978. [Google Scholar] [CrossRef] [Green Version]
- Das Gupta, S.; Suh, N. Tocopherols in cancer: An update. Mol. Nutr. Food Res. 2016, 60, 1354–1363. [Google Scholar] [CrossRef] [Green Version]
- Aghayan, M.; Asghari, G.; Yuzbashian, E.; Dehghan, P.; Haghighian, H.K.; Mirmiran, P.; Javadi, M. Association of nuts and unhealthy snacks with subclinical atherosclerosis among children and adolescents with overweight and obesity. Nutr. Metab. 2019, 16, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, H.; Healy, M.J. The graphical presentation of a collection of means. J. R. Stat. Soc. Ser. A 1995, 158, 175–177. [Google Scholar] [CrossRef]
- Payton, M.E.; Greenstone, M.H.; Schenker, N. Overlapping confidence intervals or standard error intervals: What do they mean in terms of statistical significance? J. Insect Sci. 2003, 3, 34. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Overall (n = 13,877) | Walnut Consumers (n = 933) | Other Nut Consumers (n = 5187) | No-Nut Consumers (n = 7757) | p Value c | ||
|---|---|---|---|---|---|---|
| N (Unweighted) | N (in 1000) (Weighted) | % (Weighted) | % (Weighted) | % (Weighted) | ||
| Age group | <0.0001 | |||||
| 4 to 8 years | 1439 | 38,903 | 4.5% | 41.6% | 53.9% | |
| 9 to 13 years | 1479 | 41,157 | 6.8% | 35.7% | 57.5% | |
| 14 to 18 years | 1374 | 41,637 | 5.7% | 33.4% | 60.9% | |
| 19 to 50 years | 4717 | 247,556 | 7.6% | 41.9% | 50.5% | |
| 51 to 70 years | 3376 | 156,082 | 11.6% | 47.6% | 40.8% | |
| 71 years and older | 1492 | 58,701 | 14.5% | 46.9% | 38.6% | |
| Sex | <0.0001 | |||||
| Men | 6832 | 287,249 | 7.8% | 40.8% | 51.4% | |
| Women | 7045 | 296,787 | 10.1% | 44.9% | 45.0% | |
| Race/Hispanic origin | <0.0001 | |||||
| Mexican American and Other Hispanic | 3848 | 100,466 | 5.5% | 32.5% | 62.0% | |
| Non-Hispanic White | 4644 | 355,400 | 11.0% | 47.8% | 41.2% | |
| Non-Hispanic Black | 3089 | 67,538 | 3.8% | 32.6% | 63.7% | |
| Other Race | 2296 | 60,633 | 8.3% | 43.0% | 48.7% | |
| Annual household income | <0.0001 | |||||
| less than $20,000 | 2470 | 72,634 | 4.1% | 31.3% | 64.6% | |
| $20,000 to $75,000 | 6755 | 258,406 | 8.3% | 41.3% | 50.4% | |
| $75,000 to $9999 | 1323 | 69,711 | 10.6% | 47.4% | 42.0% | |
| over $100,000 | 2428 | 153,838 | 12.3% | 50.5% | 37.2% | |
| Ratio of family income to poverty: mean ± SD or SE | 2.38 ± 1.59 a | 2.92 ± 0.06 b | 3.52 ± 0.10 b | 3.23 ± 0.06 b | 2.52 ± 0.06 b | <0.0001 |
| Education | <0.0001 | |||||
| Less than 9th grade | 3665 | 96,643 | 5.6% | 35.7% | 58.8% | |
| 9–11th grade (Incl. 12th grade with no diploma) | 1894 | 60,535 | 4.7% | 33.4% | 61.9% | |
| High school graduate/GED or equivalent | 2406 | 119,513 | 8.3% | 36.7% | 54.9% | |
| Some college or associates degree | 3029 | 149,525 | 9.6% | 43.6% | 46.8% | |
| College degree or above | 2322 | 142,650 | 13.4% | 56.6% | 30.0% | |
| Nutrients | 4–18 Years (n = 2670) | 19–50 Years (n = 2669) | 51–70 Years (n = 1711) | >71 Years (n = 707) |
|---|---|---|---|---|
| Magnesium, mg/day | ||||
| Current | 219.2 (214.2–224.2) | 270.4 (262.1–278.8) | 264.1 (255.5–272.6) | 232.4 (224.3–240.6) |
| Modeled | 263.9 (259.0–268.9) * | 315.0 (306.7–323.3) * | 308.5 (300.1–317.0) * | 277.5 (269.3–285.7) * |
| Calcium, mg/day | ||||
| Current | 941.4 (912.1–970.8) | 929.8 (897.2–962.5) | 858.5 (816.7–900.3) | 760.8 (714.4–807.2) |
| Modeled | 969.3 (940.0–998.6) | 957.1 (924.5–989.8) | 886.1 (844.4–927.8) | 788.9 (742.6–835.3) |
| Potassium, mg/day | ||||
| Current | 2070 (2019–2121) | 2438 (2365–2510) | 2509 (2430–2588) | 2289 (2212–2366) |
| Modeled | 2195 (2144–2246)* | 2561 (2489–2633) | 2633 (2554–2711) | 2414 (2337–2491) |
| Folate, µg DFE/d | ||||
| Current | 347.5 (338.2–356.8) | 369.0 (356.2–381.8) | 346.2 (334.3–358.1) | 319.2 (302.5–336.0) |
| Modeled | 375.3 (366.0–384.5) * | 396.6 (383.9–409.3) * | 373.4 (361.6–385.2) * | 346.9 (330.0–363.7) |
| Vitamin E, mg/day | ||||
| Current | 6.6 (6.4–6.8) | 7.7 (7.5–8.0) | 7.2 (6.9–7.5) | 6.6 (6.3–6.9) |
| Modeled | 6.8 (6.6–7.0) | 7.9 (7.7–8.2) | 7.4 (7.1–7.7) | 6.8 (6.5–7.1) |
| Fiber, g/day | ||||
| Current | 13.6 (13.2–13.9) | 14.7 (14.0–15.4) | 14.6 (14.0–15.2) | 13.8 (13.1–14.5) |
| Modeled | 15.4 (15.1–15.8) * | 16.6 (15.9–17.3) * | 16.5 (15.9–17.1) * | 15.7 (15.0–16.4) * |
| Omega-3 fatty acids, g/day | ||||
| Current | 1.41 (1.37–1.46) | 1.76 (1.70–1.82) | 1.66 (1.58–1.73) | 1.48 (1.38–1.58) |
| Modeled | 3.98 (3.93–4.03) * | 4.33 (4.27–4.38) * | 4.23 (4.16–4.30) * | 4.08 (3.97–4.19) * |
| Protein, g/day | ||||
| Current | 67.2 (65.4–68.9) | 82.3 (79.8–84.9) | 77.2 (74.4–80.1) | 63.9 (61.3–66.5) |
| Modeled | 71.5 (69.7–73.2) * | 86.6 (84.0–89.2) | 81.6 (78.8–84.4) | 68.2 (65.7–70.8) |
| Energy, kcal/day | ||||
| Current | 1856 (1817–1896) | 2157 (2111–2203) | 1989 (1915–2062) | 1651 (1593–1710) |
| Modeled | 2041 (2002–2081) * | 2339 (2294–2385) * | 2172 (2100–2245) * | 1838 (1780–1896) * |
| Calcium | Magnesium | Folate | Vitamin E | |||||
|---|---|---|---|---|---|---|---|---|
| Age Group | Usual Diet % (95% CI) | After Modeling % (95% CI) | Usual Diet % (95% CI) | After Modeling % (95% CI) | Usual Diet % (95% CI) | After Modeling % (95% CI) | Usual Diet % (95% CI) | After Modeling % (95% CI) |
| Boys | ||||||||
| 4–8 years (n = 424) | 33.7 (27.5–39.9) | 29.9 (23.9–35.9) | 4.4 (2.9–5.9) | 0.3 (0.1–0.5) * | 4.0 (1.5–6.5) | 1.6 (0.2–2.9) | 56.8 (51.0–62.6) | 53.5 (47.7–59.3) |
| 9–13 years (n = 452) | 66.8 (62.0–71.6) | 64.2 (59.2–69.1) | 41.2 (35.2–47.1) | 18.3 (13.7–23.0) * | 19.1 (14.7–23.6) | 12.4 (8.7–16.2) | 77.9 (74.5–81.3) | 76.5 (73.0–80.0) |
| 14–18 years (n = 456) | 64.8 (60.6–69.0) | 62.4 (57.9–66.9) | 82.7 (79.6–85.9) | 71.6 (67.6–75.6) * | 44.6 (38.8–50.4) | 37.1 (31.3–43.0) | 88.2 (85.2–91.1) | 87.5 (84.5–90.6) |
| Total (Boys) (n = 1332) | 56.0 (52.9–59.2) | 53.1 (49.9–56.4) | 45.7 (43.3–48.0) | 32.9 (30.7–35.1) * | 24.2 (20.7–27.6) | 18.4 (15.2–21.7) | 75.4 (72.7–78.1) | 73.7 (70.9–76.5) |
| Girls | ||||||||
| 4–8 years (n = 422) | 42.3 (36.9–47.8) | 38.1 (32.9–43.4) | 6.3 (4.7–7.8) | 0.4 (0.2–0.7) * | 5.6 (3.0–8.1) | 2.3 (1.0–3.6) | 59.9 (56.1–63.8) | 56.5 (52.9–60.1) |
| 9–13 years (n = 485) | 75.3 (70.7–79.9) | 72.8 (68.1–77.5) | 50.6 (45.2–55.9) | 24.3 (19.7–28.9) * | 24.5 (19.9–29.1) | 16.0 (12.3–19.7) * | 82 (78.7–85.2) | 80.6 (77.2–83.9) |
| 14–18 years (n = 431) | 82.1 (77.6–86.6) | 80.4 (75.8–85.0) | 89.0 (85.9–92.0) | 78.3 (74.6–82.1) * | 63.9 (59.1–68.7) | 55.2 (50.0–60.3) | 95.2 (92.7–97.6) | 94.8 (92.2–97.4) |
| Total (Girls) (n = 1338) | 68.1 (64.8–71.4) | 65.4 (62.1–68.6) | 51.2 (48.3–54.1) | 36.4 (33.5–39.3) * | 32.9 (29.5–36.3) | 25.8 (22.8–28.9) * | 80.2 (78.0–82.4) | 78.6 (76.4–80.8) |
| Total (Boys and Girls) (n = 2670) | 61.8 (59.2–64.4) | 59.0 (56.3–61.6) | 48.3 (46.1–50.5) | 34.6 (32.7–36.5) * | 28.3 (25.7–30.9) | 22.0 (19.5–24.4) * | 77.7 (75.7–79.7) | 76.0 (74.0–78.1) |
| Adults | ||||||||
| 19–50 years | ||||||||
| Men (n = 1367) | 35.1 (31.5–38.6) | 32.1 (28.7–35.5) | 66.0 (62.7–69.2) | 51.1 (47.4–54.7) * | 35.6 (31.7–39.5) | 28.3 (24.7–31.8) | 81.5 (78.8–84.2) | 80.7 (77.9–83.5) |
| Women (n = 1302) | 57.1 (53.0–61.2) | 53.6 (49.3–57.9) | 65.2 (61.5–69.0) | 43.4 (39.7–47.1) * | 58.4 (54.3–62.6) | 49.2 (45.2–53.2) * | 93.0 (91.5–94.5) | 92.5 (91.0–94.1) |
| Total (n = 2669) | 45.1 (41.9–48.3) | 41.9 (38.7–45.1) | 65.6 (62.7–68.6) | 47.6 (44.5–50.7) * | 46.0 (42.8–49.2) | 37.8 (34.7–40.8) * | 86.7 (84.8–88.6) | 86.1 (84.1–88.0) |
| 51–70 years | ||||||||
| Men (n = 896) | 41.0 (36.0–46.0) | 37.6 (32.8–42.4) | 73.0 (69.5–76.4) | 59.9 (56.2–63.6) * | 39.9 (36.6–43.2) | 31.8 (28.7–34.8) * | 84.8 (82.2–87.5) | 84.0 (81.3–86.8) |
| Women (n = 815) | 82.7 (78.5–87.0) | 80.9 (76.5–85.3) | 72.3 (67.7–76.9) | 51.5 (46.3–56.7) * | 65.3 (61.2–69.4) | 56.2 (51.6–60.7) * | 95.1 (92.2–98.1) | 94.8 (91.8–97.8) |
| Total (n = 1711) | 61.2 (57.2–65.3) | 58.6 (54.5–62.7) | 72.6 (70.1–75.2) | 55.8 (52.7–59.0) * | 52.2 (49.5–54.9) | 43.6 (40.6–46.6) * | 89.8 (87.8–91.8) | 89.2 (87.2–91.2) |
| >71 years (n = 707) | 81.4 (77.3–85.5) | 79.4 (74.8–84.0) | 82.8 (80.2–85.5) | 65.9 (61.9–69.9) * | 58.2 (52.3–64.2) | 48.1 (41.9–54.4) | 94.7 (93.3–96.1) | 94.3 (92.9–95.8) |
| Total (Men) (n = 2634) | 40.3 (37.4–43.1) | 37.3 (34.5–40.1) | 69.8 (67.5–72.2) | 55.9 (53.2–58.6) * | 38.0 (35.2–40.8) | 30.2 (27.5–32.9) * | 83.3 (81.4–85.2) | 82.6 (80.6–84.5) |
| Total (Women) (n = 2453) | 68.9 (65.7–72.2) | 66.1 (62.7–69.6) | 69.3 (66.5–72.1) | 47.8 (44.8–50.7) * | 61.6 (58.5–64.7) | 52.2 (49.1–55.4) * | 94.2 (92.8–95.7) | 93.8 (92.4–95.3) |
| Total (All Adults) (n = 5087) | 53.8 (51.3–56.3) | 50.9 (48.4–53.4) | 69.6 (67.4–71.8) | 52.0 (49.6–54.4) * | 49.2 (47.1–51.3) | 40.6 (38.5–42.8) * | 88.5 (87.2–89.8) | 87.9 (86.5–89.3) |
| Potassium | Fiber | |||
|---|---|---|---|---|
| Age Group | Usual Diet % (95% CI) | After Modeling % (95% CI) | Usual Diet % (95% CI) | After Modeling % (95% CI) |
| Boys | ||||
| 4–8 years (n = 424) | 31.7 (26.4–37.0) | 37.8 (32.2–43.3) | 1 (0.4–1.7) | 0.6 (0.1–1.1) |
| 9–13 years (n = 452) | 29.5 (24.9–34.0) | 34.6 (29.5–39.7) | 0.8 (0.3–1.3) | 0.5 (0.1–0.9) |
| 14–18 years (n = 456) | 20.4 (15.8–25.1) | 23.6 (18.7–28.5) | 0.4 (0.1–0.8) | 0.2 (0.0–0.5) |
| Total (Boys) (n = 1332) | 26.7 (24.0–29.5) | 31.4 (28.5–34.3) | 0.7 (0.2–1.2) | 0.4 (0.1–0.8) |
| Girls | ||||
| 4–8 years (n = 422) | 21.8 (18.1–25.4) | 27.5 (23.5–31.5) | 2 (1.0–3.0) | 1.2 (0.4–1.9) |
| 9–13 years (n = 485) | 27.8 (23.4–32.2) | 33.8 (28.9–38.8) | 1.1 (0.5–1.8) | 0.7 (0.3–1.1) |
| 14–18 years (n = 431) | 21.8 (17.1–26.4) | 26.5 (21.5–31.5) | 0.9 (0.3–1.4) | 0.5 (0.1–0.9) |
| Total (Girls) (n = 1338) | 23.9 (21.5–26.4) | 29.4 (26.7–32.0) * | 1.3 (0.6–2.0) | 0.8 (0.3–1.2) |
| Total (Boys and Girls) (n = 2670) | 25.4 (23.3–27.5) | 30.4 (28.2–32.7) * | 1 (0.4–1.6) | 0.6 (0.2–1.0) |
| Adults | ||||
| 19–50 years | ||||
| Men (n = 1367) | 22.9 (20.3–25.6) | 25.8 (22.9–28.7) | 0.4 (0.1–0.8) | 0.2 (0.0–0.5) |
| Women (n = 1302) | 22.8 (19.6–26.1) | 27.1 (23.7–30.5) | 0.7 (0.2–1.2) | 0.5 (0.1–0.8) |
| Total (n = 2669) | 22.9 (20.6–25.2) | 26.4 (23.9–28.9) | 0.6 (0.1–1.0) | 0.3 (0.1–0.6) |
| 51–70 years | ||||
| Men (n = 896) | 25.3 (21.8–28.8) | 28.2 (24.7–31.7) | 0.6 (0.1–1.2) | 0.4 (0.0–0.7) |
| Women (n = 815) | 23.9 (19.5–28.2) | 28.6 (23.9–33.3) | 1.4 (0.6–2.1) | 0.8 (0.3–1.4) |
| Total (n = 1711) | 24.6 (22.3–26.9) | 28.4 (25.9–30.9) | 1 (0.3–1.6) | 0.6 (0.2–1.0) |
| >71 years (n = 707) | 17.3 (14.5–20.1) | 21.3 (18.2–24.4) | 2.4 (1.1–3.7) | 1.7 (0.7–2.6) |
| Total (Men) (n = 2634) | 22.9 (20.9–25.0) | 25.8 (23.6–28.0) | 0.6 (0.2–1.0) | 0.4 (0.0–0.7) |
| Total (Women) (n = 2453) | 22.7 (20.5–24.9) | 27.2 (24.9–29.6) | 1.2 (0.6–1.8) | 0.8 (0.4–1.2) |
| Total (All Adults) (n = 5087) | 22.8 (21.1–24.5) | 26.5 (24.6–28.4) * | 0.9 (0.4–1.4) | 0.6 (0.2–0.9) |
| HEI Score a (Mean (95% CI)) | ||
|---|---|---|
| Age Group | Usual Diet | After Modeling |
| Boys | ||
| 4–8 years | 51.4 (48.93–53.77) | 61.4 (59.17–63.73) * |
| 9–13 years | 46.8 (44.26–49.34) | 56.4 (54.09–58.76) * |
| 14–18 years | 44.6 (42.42–46.79) | 53.3 (51.31–55.22) * |
| Total (Boys) | 47.3 (45.67–48.94) | 56.5 (55.00–58.12) * |
| Girls | ||
| 4–8 years | 54.1 (52.23–55.97) | 65.2 (63.27–67.08) * |
| 9–13 years | 51.6 (49.10–54.19) | 60.8 (58.59–63.03) * |
| 14–18 years | 48.7 (45.88–51.46) | 58 (55.62–60.41) * |
| Total (Girls) | 51.5 (50.06–53.07) | 61.1 (59.88–62.33) * |
| Total (Boys and Girls) | 49.1 (47.94–50.37) | 58.5 (57.52–59.56) * |
| Adults | ||
| 19–50 years | ||
| Men | 49.7 (47.86–51.65) | 56.2 (54.69–57.78) * |
| Women | 50.7 (48.45–53.02) | 58.4 (56.40–60.48) * |
| Total | 50.1 (48.36–51.87) | 57.1 (55.68–58.54) * |
| 51–70 years | ||
| Men | 54 (51.09–56.98) | 59.7 (57.11–62.42) * |
| Women | 56.4 (54.66–58.14) | 63.7 (62.04–65.42) * |
| Total | 55 (53.00–56.93) | 61.4 (59.52–63.32) * |
| >71 years | 59.6 (56.37–62.67) | 66.5 (63.78–69.14) * |
| Total (Men) | 51.7 (50.14–53.18) | 57.9 (56.57–59.25) * |
| Total (Women) | 53.5 (51.86–55.16) | 61.1 (59.50–62.69) * |
| Total (All Adults) | 52.4 (50.99–53.79) | 59.2 (57.95–60.50) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spence, L.A.; Henschel, B.; Li, R.; Tekwe, C.D.; Thiagarajah, K. Adding Walnuts to the Usual Diet Can Improve Diet Quality in the United States: Diet Modeling Study Based on NHANES 2015–2018. Nutrients 2023, 15, 258. https://doi.org/10.3390/nu15020258
Spence LA, Henschel B, Li R, Tekwe CD, Thiagarajah K. Adding Walnuts to the Usual Diet Can Improve Diet Quality in the United States: Diet Modeling Study Based on NHANES 2015–2018. Nutrients. 2023; 15(2):258. https://doi.org/10.3390/nu15020258
Chicago/Turabian StyleSpence, Lisa A, Beate Henschel, Rui Li, Carmen D Tekwe, and Krisha Thiagarajah. 2023. "Adding Walnuts to the Usual Diet Can Improve Diet Quality in the United States: Diet Modeling Study Based on NHANES 2015–2018" Nutrients 15, no. 2: 258. https://doi.org/10.3390/nu15020258