



Research Article
Yogendra Amatya, Amanda Helen Douglas, Nisha Devi Gurung, Aashutosh Jha
Correspondence Address :
Amanda Helen Douglas
Dept of GP, Patan Academy of Health Sciences (PAHS)
Lalitpur, P.O.Box 26500, Kathmandu
Nepal
Received on: February 23, 2021, Accepted on: March 01, 2021, Published on: March 05, 2021
Citation: Yogendra Amatya, Amanda Helen Douglas, Nisha Devi Gurung, Aashutosh Jha (2021) Barriers to Accessing Healthcare during COVID-19 LOCKDOWN: A Point Prevalence Study amongst Patients Attending Emergency and General Out-patient Clinics of PATAN HOSPITAL, NEPAL
Copyright: 2021 Amanda Helen Douglas, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Barriers to healthcare exist, particularly for poor, vulnerable patients. The coronavirus pandemic and resulting lockdowns, impacted healthcare access worldwide. January 2020, Nepal reported its first Covid-19 case, as cases increased worldwide, the government imposed a four-month lockdown. Our study evaluates the prevalence of barriers to healthcare during this lockdown.
Methods: This is an observational cross-sectional point prevalence study. All patients attending Patan Hospital’s emergency department (ED), general out-patient (OPD) and fever clinics (FC) during a 24-hour period were included. Data were collected through researcher administered, Nepali, written surveys.
Results: Data were collected from 117 participants, none declined. Hospital attendance was reduced compared to 2019. 51% participants were male, mean age 29yrs (range 0.16 - 85yrs). Most frequent attendance reasons; vaccination 17% (OPD 31%), respiratory symptoms/fever 15% (25% FC) and abdominal pain 15% (40% ED). Mean symptom duration was 6 days (4 days ED). 42% patients (50% FC) delayed attendance for; virus exposure fear 32% (47% OPD), transportation problems 23% (29% OPD) and hospital opening uncertainty 11% (21% OPD). 50% of patients (69% FC) reported difficulties; security stops 44% (55% OPD), transportation 37% (45% OPD) and financial 12% (20% FC).
Discussion: Fewer patients attended hospital than 2019 average, those attending described considerable barriers; physical, psychological and knowledge. Many experienced difficulties and delayed presenting. Transportation, security stops and financial issues were significant, potentially insurmountable barriers to vulnerable patients. Lack of public transportation and affordable ambulances must be addressed and virtual consultations considered to overcome barriers.
Psychological barriers were prevalent, with high virus exposure anxiety. Lack of knowledge surrounding hospital provision and travel regulations presented additional barriers. Dissemination of frequent, accurate information regarding services and infection control measures is vital to reassure populations.
Conclusion: Lockdowns generate significant barriers to healthcare. Governments and providers need to understand and ameliorate these to ensure access during lockdowns.
Keywords: Asia, Barriers, Covid-19, Lockdown, Nepal
List of Abbreviations
ED: Emergency Department
FC: Fever Clinic
OPD: Out Patient Department
Introduction
There are numerous and substantial barriers to accessing health care, especially for vulnerable or poor patients [1,2]. Income has been found to be one of the most significant factors in determining patients' health seeking behaviour and spending [3]. Transportation is a substantial barrier for patients’ in low and middle-income countries [4-8], constituting patients second highest healthcare cost after medication [9]. It is important, therefore, that healthcare is both financially and physically accessible [10]. The presence of barriers to patients’ accessing healthcare may result in delayed presentation and increased mortality [5,10,11].
Barriers to healthcare increased during the Covid-19 pandemic, particularly during government lockdowns when public and private transportation was restricted.
In January 2020 Nepal reported its first confirmed case of Covid-19 [12]. On 24th March the government introduced a country wide lockdown in response to the global pandemic. Public and private transport was prohibited and people were instructed to remain at home [13], except for essential shopping or accessing emergency healthcare. The lockdown was lifted after four months, on 21st July [14].
During the strict lockdown, Nepal experienced many negative impacts on health [15] including a: 200% increased maternal mortality rate [16,17], 20% increased suicide rate [18], increased reports of domestic violence [19], online bullying and abuse [20] and outbreaks of measles due to disrupted vaccination programmes [21]. Increased barriers to accessing maternal healthcare have been described, particularly lack of transportation [16,22]. Although travel for emergency healthcare during lockdown was permitted, the researchers hypothesize that this would present additional and potentially overwhelming barriers. Therefore, this study aims to assess the prevalence of barriers for patients attending Patan hospital during the Covid-19 lockdown.
Methods
This study employs quantitative methodology with an underpinning positivist paradigm. An observational crosssectional point prevalence study, designed to evaluate the prevalence of barriers for patients accessing healthcare during Covid-19 lockdown.
Study Setting
Patan Hospital in Kathmandu, is one of the largest teaching hospitals in Nepal and provides services to approximately 320 000 outpatients and 20 000 inpatients each year [23].
Patan Hospital’s mission is to “provide quality, compassionate health care to everyone who comes to the hospital, regardless of their ability to pay” [23] and it serves many of the most disadvantaged from both inside and outside of the Kathmandu valley. In 2020 Patan was designated as a Covid-19 response hospital. Throughout the pandemic it has continued to operate emergency and outpatient departments for both covid and noncovid patients, together with a newly established Fever Clinic for suspected Covid-19 cases.
Participants
The study population consisted of all patients who attended the emergency department (ED), general out-patient (OPD) and fever clinics (FC) of Patan Hospital within a single 24-hour period, from 8am on 18th May to 8am on 19th May. Patients attending specialist clinics and hospital inpatients were excluded from the study.
Ethical Consideration
Ethical approval for the study was gained from the local ethics review board prior to commencement. Participation in the study was voluntary and participants understood that they were free to decline to participate or withdraw at any time prior to data analysis. Verbal consent was taken from participants or their relatives if a child or incapacitated. Participants were assured that their identity and responses would be anonymised.
Participants understood that their responses were part of a research project and may be published. Data was collected prior to medical consultation in the outpatient (OPD) and fever clinic (FC) departments. Emergency department (ED) patients were first assessed and, if critical, treated prior to data collection. No participants’ assessment or treatment was delayed due to data collection.
Researchers observed covid-19 infection control precautions of masks or personal protective equipment as required and maintained a physical distance from participants throughout the data collection process.
Data Collection
A written paper survey was employed for data collection. The survey tool was designed by the research group after literature review and based upon questions devised by Samad et al. [11]. The survey included both open response and closed questions regarding; patient demographics, reason for presenting, duration of problem, difficulties attending, self-perception of delay and anxiety attending hospital during lockdown (see appendix 1). The survey tool was translated into Nepali and back translated into English to ensure accuracy. Data were collected in Nepali. The survey was piloted to ensure face validity. Researcher assistants were trained on data collection using the tool, to ensure consistency and standardisation of data recording. Due to low literacy levels, participants did not complete the survey tool themselves. Research assistants situated in each data collection site, completed the survey with participants.
Analysis
Open responses were analysed thematically. Quantitative data were analysed using Microsoft excel descriptive statistics and expressed as mean, standard deviation, range and percentages. Chi squared test, unpaired t-test were used as appropriate and p value of <0.05 was taken as statistically significant.
Results
All patients attending the relevant departments within the study timeframe were included, none declined to participate. Data were collected from 117 patients; 61 general OPD, 36 fever clinic and 20 emergency department.
In May 2019 Patan hospital’s monthly OPD attendance was 3547 female and 3911 males, a combined daily average of 276 patients, with clinics conducted 6 days per week. Prior to the covid lockdown separate male and female outpatient clinics were held, however, due to decreased patient load these were merged. On the study day the combined general OPD and fever clinic attendance was 97 patients, 35% of the May 2019 daily average. Total patient attendance in Patan ED in May 2019 was 4294, with a daily average of 139. On the day our study was conducted 20 patients attended the emergency department, 14% of the May 2019 daily average attendance.
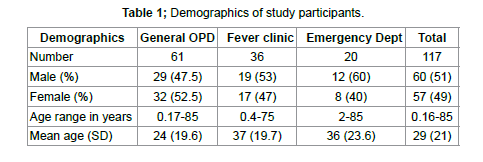
Overall (table 1) participants were almost equal in proportion of male to female (51% to 49%) with observed variations across departments not statistically significant (chi squared test statistics 0.98, p value =0.61) and variables found to be independent. There was a wide range of patients’ ages, however, the mean age was relatively young (<40 years) for each department. A large majority of patients were resident within
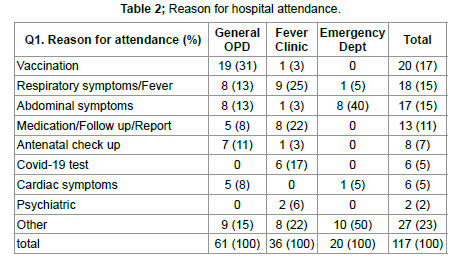
the Kathmandu valley (figure 1), with the highest proportion from outside the valley seen in fever clinic. The differences are statistically significant (chi squared test statistic 27.73, p<0.05). This was likely due to the Covid-19 risk criteria at the time of study, identifying patients from outside Kathmandu as higher risk (due to geographical Covid-19 prevalence) and hence triaging them to fever clinic rather than general OPD or ED. The commonest reason for attendance (table 2) was routine vaccination, followed by abdominal and respiratory symptoms.
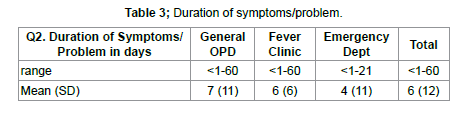
There was a wide range of duration of symptoms (table 3) for patients attending each department.
Many patients reported having delayed presentation to hospital (table 4); 50% in FC, 39% in OPD, 35% ED. The difference between the observed and expected results were statistically significant and the variables not independent (chi test stat 1.325, p value= 0.5). The difference in the duration of symptoms for those who delayed presentation was statistically significant for OPD and overall (p<0.05).
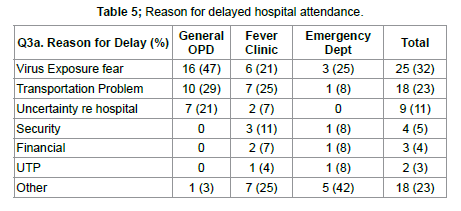
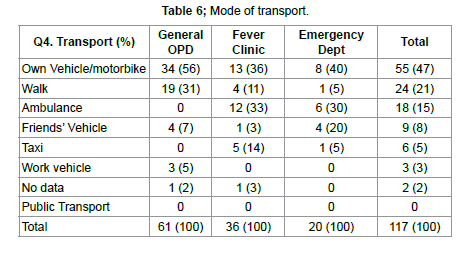
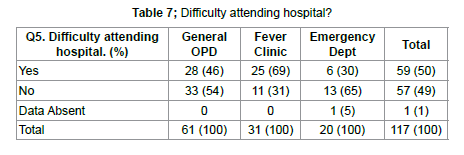
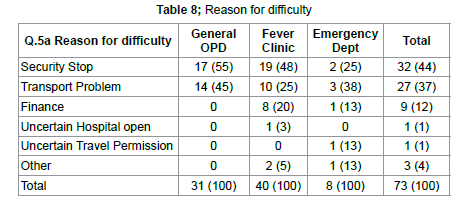
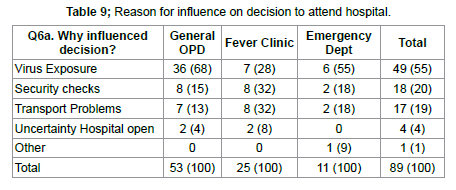
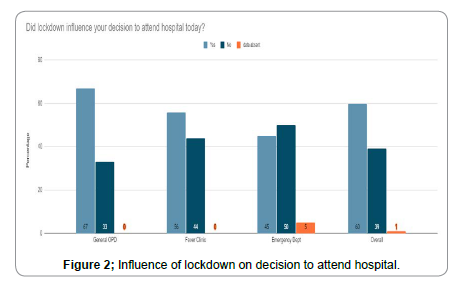
The commonest reported reason for delayed presentation to hospital (table 5) was fear of virus exposure, followed by transportation problems. The majority of patients attended hospital (table 6) in their own car or motorbike (47%), although 31% of OPD and 21% of all patients walked to hospital. 30% of ED patients travelled by ambulance. There was no public transport on the day of study due to lockdown regulations. 50% of patients reported difficulty attending hospital (table 7), with fever clinic patients reporting the highest levels of difficulty (69%) and ED patients’ the lowest (30%) (Test stat 8.4, p value=0.015) these were not found to independent variables and the difference was statistically significant. This may be explained by the higher use of ambulances among ED patients. A large proportion of patients (44% overall) reported facing a security check/stop whilst travelling to hospital (table 8); 55% OPD, 48% fever clinic, although this was less for ED patients (25%), likely related to their higher ambulance usage (ambulances are exempt from most security stops). The second most commonly encountered problem was transportation, 37% overall, 45% OPD, 25% FC and 38% ED. Overall 60% of patients reported that the lockdown did influence their decision on whether to attend hospital, this rose to 67% for OPD (figure 2), however, the observed difference was not statistically significant (Chi Sq test stat 2.884, p value= 0.24). The main reason given by patients influenced in their hospital attendance was the fear of virus exposure (55% overall). Concerns surrounding security checks and transportation problems were also evident in almost 20% of patients (table 9). A large majority of patients felt anxious attending hospital (74% overall), particularly those attending FC (83%). Lowest anxiety levels reported amongst ED patients (50%), with these observed differences found to be statistically significant (Chi test stat 6.54, p value <0.05).
The most frequently cited reason for anxiety (table 10) was the fear of virus exposure (82% overall), seen across all departments. Surprisingly few participants reported anxiety regarding security checks (8% overall) or transportation (highest for ED patients 17%).
Discussion
Our study shows a drastically reduced hospital attendance on the study day, in both the OPD and emergency departments, compared to the previous year. The patients who attended hospital described considerable barriers to accessing healthcare; physical, psychological and knowledge. Many patients reported facing difficulties attending and reported delaying their presentation to hospital.
Psychological barriers were frequently described, with the fear of contracting covid-19 the most prevalent. The impact of this is seen in the high proportion of patients who identified it as their reason for delaying hospital presentation, and as having influenced their decision on attending hospital.
Physical barriers to accessing healthcare were also described by participants. Half of the patients reported difficulties due to transportation, security stops and financial problems. Almost half the study participants travelled to hospital in their own vehicle (motorbike or car), 21% walked. Vehicle ownership in a low-to-middle-income country like Nepal is low; with 6 cars and 66 motorbikes per 1000 population [24]. Nepal’s lockdown regulations at the time of the study, prohibited all public transportation including taxis. It is likely that the majority of patients who presented to hospital were from higher socioeconomic groups, having access to their own vehicle, or lived near enough to the hospital to walk. Private vehicle movement was permitted for medical purposes; however, police security stops, frequently experienced by our patients, may have deterred others from attending. Ambulances were permitted to travel during lockdown largely without security checks and were mostly employed by ED patients. Ambulances in Nepal are private and expensive to use, with media reports of price inflation during lockdown [25], this presents an additional financial barrier. Clearly transportation issues impacted patients’ health seeking behaviour, with many citing it as the reason behind delayed presentation.
Whilst the cessation of public transport during lockdown was arguably a difficult but necessary measure to reduce coronavirus spread, the negative impact of such decisions needs to be clearly understood and, if possible, mitigated against. In many countries’ healthcare providers have adapted to the pandemics restrictions by offering remote, virtual medical consultations, either via telephone or online. Some have described this rapid development as a long awaited “game changer” [26,27] and unintended positive result of pandemic distancing on medical consultations [28]. This is not a comprehensive solution, as patients report it is a satisfactory alternative during the pandemic but inferior to face to face interactions [29]. A major concern, however is the lack of equal access to virtual/remote consultations, due to financial, educational, geographical and infrastructure factors [30-33]. This may result in additional healthcare barriers for those patients arguably most in need of care; poor, least educated, rural and vulnerable [31,33], particularly in developing nations [30]. Whilst this is not appropriate or viable for all consultations or patients, particularly the most vulnerable [34], governments should consider addressing some of the regulatory obstacles to facilitate it’s wider implementation [33]. It is important that providers and governments look creatively at ways to ensure access to healthcare when implementing lockdown regulations. Strengthening telecommunication and internet access plus digitalising medical records makes virtual consultations a more viable alternative. Not all medical consultations, however, can be undertaken remotely, some patients will need to attend facilities. Authorities must ensure safe, affordable transportation is available to those without their own vehicle. This could, potentially be achieved through the expansion and subsidising of ambulance services.
Psychological barriers to healthcare during lockdown were considerable and require targeted responses to overcome them. Patients need to be confident that healthcare facilities have implemented infection control measures that are robust enough to prevent virus transmission to and between patients. Public health workers have an important role to play in reassuring and building confidence in those needing to access services. The development and dissemination of clear and accessible communication, information and education (ICE) materials is vital for relieving health seekers anxiety [35]. Such communication should be shared across a variety of media to increase their reach and impact.
Lack of knowledge as a barrier to healthcare was seen in a small but important proportion of patients. They described their uncertainty about whether hospital services were open and travel for medical care was permissible as contributing to their; delayed presentation, access difficulties and the decision to attend. There is a need for increased public awareness and education regarding medical service provision and access during lockdown, through clear public health and media communication.
Encouragingly our study showed a high proportion of general OPD visits for routine vaccination. Many local healthcare centers halted vaccination services during lockdown, forcing parents to either attend hospital for their child’s vaccination or delay and potentially miss the dose. This may have resulted in the higher proportion of vaccine attenders seen in our study, due to lack of alternative provision. It should be noted, however, that widespread disruption in vaccine delivery has resulted in measles outbreaks across the country [21]. Despite a high proportion of vaccination visits, overall OPD attendance, however, was reduced. Public health officials need to consider the impact of lockdown on delivery of vaccinations for preventable infectious diseases. There needs not only to be a swift resumption of vaccination services but also considerable effort and education to ensure catchup vaccines for those negatively impacted, to prevent further outbreaks. The main limitation of our study is that it only includes those who were able to attend hospital. It is possible that patients who did not attend faced different barriers, indeed insurmountable barriers, than those described. It was not feasible to include these individuals in the study population. The relatively short duration of data collection, over only 24hours, and resulting small sample size means that it may not be truly reflective of hospital attendances. Qualitative research would enable a richer exploration and understanding of barriers faced by patients and would be an avenue of potential future study.
Conclusion
Lockdown has been used as a tool for controlling virus transmission in many countries across the world, but it’s impact on those trying to access healthcare in Nepal had not been clearly understood. Lockdown is a blunt tool, creating many unintended barriers to healthcare as seen in our study. Nepal has come through its first pandemic wave, although not without significant casualties and currently has only clusters of cases [36]. Unfortunately, the picture in other countries paints the likelihood of a second wave of infections yet to arrive [37], and with it potentially more lockdowns [38]. It is vital that government decision makers, public health departments and healthcare providers learn lessons from the first pandemic lockdown and strive to reduce the barriers to accessing healthcare for all.
Declarations
Ethics approval and consent to participate Informed verbal consent was taken from all study participants. Their participation was voluntary and they were free to decline to participate or withdraw consent prior to data analysis. Participants were aware that all data was anonymous and they would not be identified in analysis or publication. Ethical approval was obtained prior to the study’s commencement, from Patan Academy of Health Sciences IRC.
Consent for publication
The authors declare they have no competing interests.
Availability of Data and Materials
The data set used and/or analysed during the current study are available from the correspondence author on reasonable request.
Competing Interests
The authors declare that they have no competing interests.
Funding
None
Authors contributions
YA and AHD were involved in the study conceptualisation and establishing the methodology. AJ and NDG collected the data. AHD analysed and interpreted the data. YA and AHD wrote the original draft of the manuscript. All authors read and approved the final manuscript.
1. Sachs J. Macroeconomics and health: investing in health for economic development. Report of the Commission on Macroeconomics and Health. Geneva: World Health Organization. 2001.
2. McNamee P, Ternent L, Hussein J. Barriers in accessing maternal healthcare: evidence from low- and middle-income countries. Expert Review of Pharmacoecon Outcomes Res. 2009;9(1): 41-48.
3. Gerdtham U, Jonsson B. International comparisons of health expenditure: theory, data and econometric analysis. In: Culyer J, Newhouse JP (eds). Handbook of health economics: volume 1A. Amsterdam: North-Holland 2000.
4. Ensor T. (1996) Health sector reform in Asian transition countries: study on social sector issues in Asian transition economies. York: University of York, for the Asian Development Bank.
5. Fawcus S, Mbizvo M, Lindmark G, Nystrom L. A community-based investigation of avoidable factors for maternal mortality in Zimbabwe. Stud Fam Plann. 1996;27(6): 319–27.
6. Rankin SL, Hughes-Anderson W, House AK, et al. Costs of accessing surgical specialists by rural and remote residents. ANZ J Surg. 2007;71(9): 544–547.
7. Segall M, Tipping G, Lucas H, Dung TV, Tam NT, et al. Health care seeking by the poor in transitional economies: the case of Vietnam. Sussex, UK: Institute of Development Studies; Feb 2000.
8. Anonymous. Pakistan demographic health Survey 2006–07. National Institute of Population Studies and Macro International Inc., Islamabad 2008.
9. CIET Canada. (2000) Service Delivery Survey: second cycle, 2000 preliminary findings. Dhaka: Health and Population Sector Programme.
10. Ensor T, Cooper S. Overcoming barriers to health service access: influencing the demand side. Health Policy Plan. 2004;19(2): 69-79.
11. Samad L, Jawad F, Sajun SZ, Arshad MH, Baig-Ansari N. Barriers to Accessing Surgical Care: A Cross-Sectional Survey conducted at a Tertiary Care Hospital in Karachi, Pakistan. World J Surg. 2013;37(10): 2313-21.
12. Bastola A, Sah R, Rodriguez-Morales AJ, et al. The first 2019 novel coronavirus case in Nepal. The Lancet Infectious Diseases. 2020;20(3):279-280.
13. Pradhan, TR. (2020) Nepal goes under lockdown for a week starting 6am Tuesday. Kathmandu Post. 23 March. https://kathmandupost.com/national/2020/03/23/nepal-goes-under-lockdown-for-a-week-starting-6amtuesday
14. Pradhan, TR. (2020) Government decides to lift the four-month-long coronavirus lockdown, but with conditions. The Kathmandu Post. 22 July.
15. Mahato P, Tamang P, Shahi P, et al. Europasian Journal of Medical Sciences. Effects of Covid-19 during lockdown in Nepal. 2020; 2(2): covid-19 Special Issue 3.
16. One Heart Worldwide. (2020) COVID-19 updates and One Heart Response, Accessed 29 May 2020.
17. Poudel A. A 200 percent increase in maternal mortality since the lockdown began. The Kathmandu Post. 2020; 27 May.
18. Neupane A. Suicide cases on the rise, mental health experts warn of a ‘grim situation’. My Republica 2020; 21 May.
19. WOREC. (2020) 336 Cases of Violence Against Women and Girls Committed During Lockdown, 2020.
20. Save The Children. (2020) COVID-19: Millions of children in lockdown in Asia at risk of domestic violence.
21. UNICEF. (2020) Disruption of child vaccination in South Asia poses an urgent threat to children’s health-UNICEF. Accessed 02 June 2020.
22. UNFPA. (2020) In Nepal, COVID-19 turning pregnancy excitement into fear. Accessed May 12, 2020.
23. Patan Hospital Nepal. Website; https://www.pahs.edu.np/pahs-community/hospital/
24. Neupane N. (2018) Trend of automobile ownership. The Kathmandu Post. https://kathmandupost.com/opinion/2018/02/11/trend-of-automobileownership
25. Aryal A. (2020) Arbitrary ambulance service rates have hit people in emergency needs during lockdown. The Kathmandu Post. May 19.
26. Robbins T, Hudson S, Ray P, Sankar S, Patel K, et al. (2020) COVID-19: a new digital dawn? Digital health. 6: 2055207620920083.
27. Hollander JE, Carr BG. Virtually perfect? Telemedicine for Covid-19. N Engl J Med. 2020;382(18):1679-1681.
28. Hakim AA, Kellish AS, Atabek U, et al. Implications for the use of telehealth in surgical patients during the COVID-19 pandemic. Am J Surg. 2020;220(1):48-49.
29. Sorensen MJ, Bessen S, Danford J, et al. Telemedicine for Surgical Consultations-- Pandemic Response or Here to Stay? A Report of Public Perceptions. Ann Surg. 2020;272(3): e174-e180.
30. Okereafor K, Adebola O, Djehaiche R. Exploring the potentials of telemedicine and other non-contact electronic health technologies in
controlling the spread of the novel coronavirus disease (COVID-19). IJITE. 2020;8(4): 1–13.
31. Correa T, Pavez, I. Digital inclusion in rural areas: A qualitative exploration of challenges faced by people from isolated communities. Journal of Computer- Mediated Communication. 2016;21(3): 247-263.
32. Smith AC, Thomas E, Snoswell C, et al. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020;26(5):309-313.
33. Leite H, Hodgkinson IR, Gruber T. New development: ‘healing at a distance’- telemedicine and COVID-19. Public Money Manag. 2020;40(6):4 83-485.
34. Christianson J, Christianson E. White paper: using telehealth in the emergency department to minimize risk to health care providers and
conserve resources during the COVID-19 response. InDoc, PA: 1–4, 2020.
35. Information, Education and Communication. (2001) Lessons from the past; perspectives for the future. WHO.
36. WHO situation Report.2nd Feb 2020. https://covid19.who.int/table
37. Hazem Y, Natarajan S, Berikaa E. Hasty reduction of COVID-19 lockdown measures leads to the second wave of infection. medRxiv. 2020;Jan 1.
38. Nazareth J, Minhas JS, Jenkins DR, et al. Early lessons from a second COVID-19 lockdown in Leicester, UK. The Lancet. 2020;Jul 18; 396(10245): e4-5.




Clinical Microbiology & Case Reports

Women's Health & Gynecology

Journal of Global Diabetes & Clinical Metabolism

Journal of Alzheimers Parkinsonism and Dementia

Journal of Dental and Oral Health

Journal of Ophthalmology & Visual Neuroscience

Cancer Science: Open Access

Journal of Immunology, Infection & Inflammatory Diseases

Journal of Prevention & Treatment of HIV/AIDS

Journal of Primary Health Care & General Practice

Journal of Blood Disorders Symptoms and Treatments

Journal of General and Emergency Medicine

Journal of Clinical Anesthesia and Pain Medicine

Journal of Applied Physics & Nanotechnology

Journal of Advances in Breast Cancer Research and Development

Interdisciplinary Journal of Gastroenterology, Hepatology and Endoscopy

Journal of General Surgery

Journal of Global Vaccines R&D

Journal of Integrative Pediatric Healthcare: Open Access

SOA-Clinical & Medical Case Reports, Reviews

Interdisciplinary Journal of Bone Marrow & Stemcell

Interdisciplinary Journal of Nursing and Critical Care

Global Journal of Internal Medicine

Journal of Integrative Food Sciences & Nutrition

Integrative Clinical Cardiology

Clinical Dermatology and Investigations

Molecular Medicine: Current Aspects
Open Access Journal of Public Health (ISI Indexed)

Annals of Clinical Research and Trials

Global Chemical Engineering & Process Technology

Integrative Plant Science & Molecular Biology

Interdisciplinary Journal of Translational Science

Integrative Neurology and Stroke

Journal of Vascular Diseases and Therapy

Integrative Trauma and Emergency Medicine

SOA-Otolaryngology-ENT Research

Global Urology and Nephrology

Journal of Pregnancy and Newborncare

SOA-Applied Biotechnology & Bioengineering

Journal of Obesity Treatment and Weight Management

SOA Medical Research & Clinical Practice

Integrative Clinical Pathology

Global Toxicology

Dairy Science, Veterinary and Animal Husbandry

SOA Radiology & Radiation Therapy

Global Analytical Techniques & Pharmaceutical Research

Abnormal Psychology and Clinical Psychiatry

SOA Archives of Pharmacy & Pharmacology

Global Nutrition and Dietetics

Global Hydrologic Engineering Research

Global Physical Medicine & Rehabilitation Practices

Integrative Oral care and Craniofacial Research
Integrative Ecology and Environmental Sciences

Open Access Journal of Sociology
Interdisciplinary Journal of Fisheries and Aquaculture research
Biomedical Research and Clinical Studies

Clinical Epidemiology and Healthcare

Molecules Research & Analysis
Journal of Polymers Research










 Open Access
by Scient Online is licensed.
Open Access
by Scient Online is licensed.

