Efficacy, acceptability, and safety of muscle relaxants for adults with non-specific low back pain: systematic review and meta-analysis
BMJ 2021; 374 doi: https://doi.org/10.1136/bmj.n1446 (Published 08 July 2021) Cite this as: BMJ 2021;374:n1446
- Aidan G Cashin, doctoral student12,
- Thiago Folly, research assistant1,
- Matthew K Bagg, doctoral student123,
- Michael A Wewege, doctoral student14,
- Matthew D Jones, lecturer14,
- Michael C Ferraro, doctoral student14,
- Hayley B Leake, doctoral student5,
- Rodrigo R N Rizzo, doctoral student14,
- Siobhan M Schabrun, associate professor1,
- Sylvia M Gustin, associate professor16,
- Richard Day, professor, medical doctor78,
- Christopher M Williams, associate professor910,
- James H McAuley, professor14
- 1Centre for Pain IMPACT, Neuroscience Research Australia, Sydney, NSW, Australia
- 2Prince of Wales Clinical School, University of New South Wales, Sydney, NSW, Australia
- 3New College Village, University of New South Wales, Sydney, NSW, Australia
- 4School of Health Sciences, Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia
- 5IIMPACT in Health, University of South Australia, Adelaide, SA, Australia
- 6School of Psychology, Faculty of Science, University of New South Wales, Sydney, NSW, Australia
- 7Clinical Pharmacology and Toxicology, St Vincent’s Hospital, Sydney, NSW, Australia
- 8St Vincent’s Clinical School, Faculty of Medicine, University of New South Wales, Sydney, NSW, Australia
- 9School of Medicine and Public Health, University of Newcastle, Callaghan, NSW, Australia
- 10Population Health, Hunter New England Local Health District, Newcastle, NSW, Australia
- Correspondence to: J H McAuley Neuroscience Research Australia, Randwick, NSW, Australia j.mcauley{at}neura.edu.au (or @pain_neura on Twitter)
- Accepted 3 June 2021
Abstract
Objective To investigate the efficacy, acceptability, and safety of muscle relaxants for low back pain.
Design Systematic review and meta-analysis of randomised controlled trials.
Data sources Medline, Embase, CINAHL, CENTRAL, ClinicalTrials.gov, clinicialtrialsregister.eu, and WHO ICTRP from inception to 23 February 2021.
Eligibility criteria for study selection Randomised controlled trials of muscle relaxants compared with placebo, usual care, waiting list, or no treatment in adults (≥18 years) reporting non-specific low back pain.
Data extraction and synthesis Two reviewers independently identified studies, extracted data, and assessed the risk of bias and certainty of the evidence using the Cochrane risk-of-bias tool and Grading of Recommendations, Assessment, Development and Evaluations, respectively. Random effects meta-analytical models through restricted maximum likelihood estimation were used to estimate pooled effects and corresponding 95% confidence intervals. Outcomes included pain intensity (measured on a 0-100 point scale), disability (0-100 point scale), acceptability (discontinuation of the drug for any reason during treatment), and safety (adverse events, serious adverse events, and number of participants who withdrew from the trial because of an adverse event).
Results 49 trials were included in the review, of which 31, sampling 6505 participants, were quantitatively analysed. For acute low back pain, very low certainty evidence showed that at two weeks or less non-benzodiazepine antispasmodics were associated with a reduction in pain intensity compared with control (mean difference −7.7, 95% confidence interval−12.1 to−3.3) but not a reduction in disability (−3.3, −7.3 to 0.7). Low and very low certainty evidence showed that non-benzodiazepine antispasmodics might increase the risk of an adverse event (relative risk 1.6, 1.2 to 2.0) and might have little to no effect on acceptability (0.8, 0.6 to 1.1) compared with control for acute low back pain, respectively. The number of trials investigating other muscle relaxants and different durations of low back pain were small and the certainty of evidence was reduced because most trials were at high risk of bias.
Conclusions Considerable uncertainty exists about the clinical efficacy and safety of muscle relaxants. Very low and low certainty evidence shows that non-benzodiazepine antispasmodics might provide small but not clinically important reductions in pain intensity at or before two weeks and might increase the risk of an adverse event in acute low back pain, respectively. Large, high quality, placebo controlled trials are urgently needed to resolve uncertainty.
Systematic review registration PROSPERO CRD42019126820 and Open Science Framework https://osf.io/mu2f5/.
Introduction
Low back pain is a major global public health problem, placing a burden on individuals, healthcare, and society, and has been the leading cause of disability worldwide for the past 30 years.1 In the United States, low back pain is responsible for the highest total expenditure on healthcare—in 2016 estimated to be $134.5bn (£95.0bn; €110.5bn) (95% confidence interval $122.4bn to $146.9bn).2 Low back pain is a common reason to visit a general practitioner,34 when patients are often prescribed analgesics to manage their symptoms.567
Muscle relaxants, a broad class of drugs that include non-benzodiazepine antispasmodics and antispastics (table 1), are frequently prescribed in the UK and US. In 2020, prescriptions in England exceeded 1.3 million,11 and in the US more than 30 million prescriptions of muscle relaxants were recorded for ambulatory care visits in 2016.12 Muscle relaxants are the third most commonly prescribed drug for low back pain.57912 Recommendations for the use of muscle relaxants have, however, conflicted between international clinical practice guidelines for low back pain.1113 For example, the US guideline recommends non-benzodiazepine antispasmodics as the drug of choice for acute low back pain,14 the Belgian guideline discourages such use,15 and the UK guideline does not make a recommendation.16
Overview of muscle relaxants* grouped according to clinical utility
A systematic review that included five randomised controlled trials (n=497 participants) published up to end of October 2015 provides the most recent evidence that muscle relaxants produce a clinically meaningful reduction in pain intensity for people with acute low back pain (mean difference −21.3, 95% confidence interval −29.0 to −13.5).17 Several large randomised controlled trials have since been published. Furthermore, this systematic review did not include evidence from randomised controlled trials in clinical trial registries, which might lead to an overestimation of the effect.18 To address this knowledge gap, we systematically reviewed the evidence to estimate the efficacy, acceptability, and safety of muscle relaxants compared with placebo, usual care, or no treatment in adults with low back pain. We evaluated the certainty of the evidence supporting the findings using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach1920 and discuss its clinical relevance.
Methods
We followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) reporting guideline.21 Supplementary file 1 shows the protocol deviations.
Data sources and searches
We searched Medline, Embase, CINAHL, the Cochrane Central Register of Controlled Trials (CENTRAL), the Cochrane Back and Neck Group’s trial register (through CENTRAL), ClinicalTrials.gov, the EU Clinical Trials Register, and the World Health Organization’s International Clinical Trial Registry Platform from inception to 23 February 2021. The search strategies were developed and piloted by the review team for bibliographic databases and clinical trial registries using medical subject headings or Emtree and text words for “low back pain”, “randomised controlled trials”, and “spasmolytic muscle relaxant medicines” (see supplementary files 2 and 3). We searched the reference lists from retrieved full text articles and previous systematic reviews. Searches were also done through PROSPERO for any ongoing or recently completed systematic reviews.
Eligibility criteria
Records of randomised controlled trials were included that allocated adults (≥18 years) with non-specific low back pain22 to receive a systemically administered dose of a spasmolytic muscle relaxant8 compared with a non-active control group (sham (placebo) drug, continuation of usual care, waiting list, or no treatment). We also included randomised controlled trials that investigated the combination of two drugs compared with one drug alone (eg, tizanidine and ibuprofen versus ibuprofen). Drugs had to be classified as muscle relaxants, listed on the WHO Anatomical Therapeutic Chemical (ATC) classification system,23 and licensed in the US (Food and Drug Administration24), Europe (European Medicines Agency25), or Australia (Australian Register of Therapeutic Goods26) as at 29 March 2019 (see supplementary file 4). Trials reported in English, Italian, Portuguese, Spanish, German, and Dutch were included. We did not restrict the inclusion of trials by the duration of low back pain reported, trial publication status, outcomes reported, or instrument used to assess outcomes. Trials were excluded that investigated suspended muscle relaxants or those not currently licensed in the US, Europe, or Australia, reported in other languages, and sampled participants with specific spinal conditions (eg, infection, neoplasm, inflammatory disease, or fracture)22 or with sciatica.27 We excluded trials that sampled multiple health conditions unless separate data were available for the participants with non-specific low back pain.
Study selection
The review team independently screened the titles and abstracts of all identified records in duplicate. We retrieved full length records of those deemed eligible and screened these again to confirm inclusion. The full length record of a trial registration was defined as the primary web page and all subsidiary pages and files located on the trial registry. Disagreements were resolved through discussion (AGC, MAW, MDJ, MCF, HBL, RRNR) or, when necessary, consultation of a third independent reviewer (MKB or JHM). When further information was required to confirm eligibility, we contacted authors up to three times within a six week period.
In instances where a trial was linked to multiple record sources, we used an established hierarchy, giving preference to the main published trial report, followed by other published records of the trial (eg, conference abstracts), and, lastly, the trial registry record. When no evidence of publication was found, we classified the trial registry record as the primary record.
Outcomes
The choice of outcomes was based on the core outcome domains for clinical trials in low back pain28 and those of other reviews of analgesics for low back pain.293031 The primary outcomes were pain intensity and acceptability (satisfaction with the treatment regimen measured by the number of patients who discontinued treatment for any reason). Secondary outcomes were disability, adverse events (as defined by each study), serious adverse events (as defined by each study), and withdrawal from treatment because of adverse effects (tolerability).
Data extraction
Using a standardised, piloted form, two reviewers independently extracted data on the trial characteristics, participants, interventions, comparisons, and outcomes from each trial. In the absence of data, we transformed or estimated measures of variance using the recommendations from section 6.5.2 in the Cochrane Handbook for Systematic Reviews of Interventions.32 Briefly, we transformed standard errors or 95% confidence intervals for group level estimates to standard deviations using equations from section 6.5.2.2.32 If studies reported mean differences between groups and P values, we calculated the between group standard error using equations from section 6.5.2.3, and used the between group estimates in the meta-analysis.32 When no measure of variance was reported, a conservative standard deviation of 30 was imputed. We resolved disagreements for data extraction through discussion, or with arbitration by a third reviewer if necessary. When data were not reported in the trial, we contacted authors up to three times over a period of six weeks.
Risk of bias and certainty of evidence
Two independent reviewers appraised study level risk of bias using the Cochrane risk of bias tool33 and recommendations from Furlan et al.34 Thirteen criteria were assessed across the risk of bias domains selection, performance, attrition, detection, reporting, and other sources of bias.34 Because recommendations were not available from Furlan et al,34 we used previously published criteria to determine overall study risk of bias for each trial.35 Two reviewers independently determined certainty of the evidence for each analysis using the GRADE system.1920 Certainty of the evidence is best considered as the certainty that the true effect lies within a particular range.36 We downgraded the certainty of evidence if a serious flaw was present in the domains of risk of bias, inconsistency, imprecision, and publication bias (see supplementary file 5). The certainty of evidence was initially classified as high then as moderate, low, or very low certainty. High certainty meant that we were very confident that the true effect was close to that of the estimate of the effect. Moderate certainty meant that we were moderately confident in the effect estimate; the true effect was likely to be close to the estimate of the effect but with a possibility of being substantially different. Low certainty meant that we had limited confidence in the effect estimate; the true effect might be substantially different from the estimate of the effect. Very low certainty meant that we had very little confidence in the effect estimate; the true effect was likely to be substantially different from the estimate of effect.19 Disagreements between appraisals of risk of bias and certainty of evidence were resolved through discussion, or, when required, by arbitration with a third reviewer.
Data synthesis and analysis
We conducted meta-analyses of trials for each outcome using the available data for immediate term (≤2 weeks post-randomisation) and short term (3-13 weeks post-randomisation) follow-up. When data for multiple time points were available for short term follow-up, we chose the time closest to six weeks. All analyses were stratified by the clinical utility of the muscle relaxant (antispastic, non-benzodiazepine antispasmodic, benzodiazepine, and miscellaneous) and the duration of low back pain observed in the included trials; acute (0-6 weeks), subacute (6-12 weeks), chronic (>12 weeks), and mixed (participants with multiple durations for symptoms). To incorporate trials with multiple comparisons, we followed guidance,32 dividing the control group sample size by the number of trial arms. As benchmarks for clinically important effects are usually expressed on a 0-100 scale,3738 and to facilitate clinical interpretation of results,39 we converted aggregate outcome data (measure of central tendency and dispersion) for pain and disability to a common 0 (no pain or disability) to 100 (worst pain or disability) scale. We divided the mean and variability measures by the top number of scale and multiplied by 100—for example, 0-24 Roland-Morris Disability Questionnaire score divided by 24 and multiplied by 100. Supplementary files 6 and 7 provide details on the pain and disability measures used by the studies, and conversion procedures. We considered a difference in favour of muscle relaxants of at least 10 points for pain and disability to be the minimal clinically important effect.3940 This threshold has been used in other reviews of analgesics for low back pain.293141
Random effects meta-analytic models were fit through restricted maximum likelihood estimation, using dmetar in R (version 3.6.1).42 We expressed effects for continuous outcomes with the mean between group difference and accompanying 95% confidence intervals, and effects for binary outcomes using the relative risk and accompanying 95% confidence intervals. The Q statistic and the between study variance (τ2) were estimated from each analysis and these values were used to calculate 95% prediction intervals for the pooled effect and I2 values. We used these measures to form judgments about heterogeneity in conjunction with visual inspection of the distribution of effect sizes in the forest plots. We formed judgments about publication bias for each meta-analysis by visually inspecting funnel plots and considering the proportion of trials included from trial registry records for that outcome.
Planned investigation of heterogeneity
We conducted a planned subgroup analysis to explore whether heterogeneity varied by prescribed dose. The dose comprised three levels: standard dose, more than standard dose, or less than standard dose, according to the Prescribers Digital Reference,43 Monthly Index of Medical Specialties,44 or Australian Medicines Handbook.45
Sensitivity analyses
We conducted sensitivity analyses to assess the influence on effect estimates of trials with unclear definitions of non-specific low back pain, trials where measures of variance were imputed, trials at high risk of bias, trials reported as trial registry records, trials without a placebo comparison, and trials investigating muscle relaxants less commonly prescribed, including carisoprodol and thiocolchicoside. This was done by repeating the main analyses without the relevant trials included.
Patient and public involvement
No patients or members of the public were directly involved in this study because of a lack of funding, although we did speak to patients about the study and we asked a member of the public to read our manuscript after submission. We plan to disseminate the results of this review to the relevant patient organisations.
Results
Overall, 3362 records were identified, 215 duplicates removed, and 3147 records screened during title and abstract screening. Forty nine trials were included in the review: 35 were peer reviewed journal articles,46474849505152535455565758596061626364656667686970717273747576777879808182 two were conference abstracts,5774 and 12 were trial registry records838485868788899091929394 (fig 1 and supplementary file 8). Thirty one trials (two trial registry records and one conference abstract), including a total of 6505 participants, contributed data to the meta-analyses.

{kind=link}
Study characteristics
The included trials investigated 18 different muscle relaxants, most commonly non-benzodiazepine antispasmodics (n=29), miscellaneous (n=11), antispastics (n=5), and benzodiazepines (n=4). The muscle relaxants investigated were administered orally in 35 trials, by intramuscular injection in 10 trials, and by intravenous injection in one trial. In three trials the drugs were administered in a mixed manner, by intramuscular injection and subsequent oral doses. Most trials (n=32) compared a muscle relaxant with placebo.
Thirty five trials sampled participants with acute low back pain, two trials sampled participants with subacute low back pain, and eight trials sampled participants with chronic low back pain. Two trials investigated participants with both acute and subacute low back pain (mixed duration sample) and two trials did not report the duration of low back pain.
Risk of bias
Of the 39 completed trials assessed for overall risk of bias, eight were assessed at low risk, three at moderate risk, and 28 at high risk. The most common reasons for being at high risk were from attrition bias (failure to report intention-to-treat effects (n=8)), performance bias (inadequate blinding of participants (n=6) or care providers (n=7)), and detection bias (inadequate blinding of outcome assessors (n=6)). There was also unclear risk of selection bias from inadequate reporting of allocation concealment (n=33) and random sequence generation (n=25) (see supplementary file 9).
Qualitative synthesis for primary outcome pain intensity (≤2 weeks)
A total of 25 included trials were unsuitable for meta-analysis of the primary outcome pain intensity. Eight trial registry records8384858687919293 provided no data and 17 peer reviewed journal articles4849505660616365667071737479808182 did not provide data for relevant treatment effects. Supplementary file 10 provides full details of these trials. For the trials that did not report relevant treatment effects for meta-analysis, 11 sampled participants with acute low back pain, five with chronic low back pain, and one did not report the duration of low back pain.
Five trials concluded that non-benzodiazepine antispasmodics were superior to control for acute low back pain,4849566374 whereas two trials found no difference.7379 Two trials concluded that antispastics were superior to control.8082 One trial concluded that benzodiazepines were superior to control,66 whereas one trial found no difference.60
Four trials50616581 concluded that miscellaneous muscle relaxants (ie, botulinum toxin) were superior to control for chronic low back pain, and one trial71 concluded that benzodiazepines were superior to control for pain intensity in the supine position but not while sitting.
Finally, one trial70 that did not report the duration of low back pain concluded that antispastics were not superior to control.
Efficacy and acceptability
Acute low back pain—Seventeen trials (24 comparisons) determined the efficacy of muscle relaxants for acute low back pain at immediate (≤2 weeks) follow-up and four trials (seven comparisons) at short term (3-13 weeks) follow-up. Thirteen trials (16 comparisons) determined the acceptability of muscle relaxants for acute low back pain. Non-benzodiazepine antispasmodics were associated with a reduction in pain intensity at two weeks or less compared with control (mean difference −7.7, 95% confidence interval −12.1 to −3.3; 16 trials, 4546 participants; very low certainty evidence) (fig 2 and table 2). Non-benzodiazepine antispasmodics were not associated with a reduction in pain intensity compared with control at 3-13 weeks (0.6, −4.5 to 5.7; 3 trials, 612 participants; moderate certainty evidence) or disability at two weeks or less (−3.3, −7.3 to 0.7; 7 trials, 2438 participants; very low certainty evidence) and 3-13 weeks (4.3, −1.4 to 10.1; 2 trials, 422 participants; moderate certainty evidence) (table 2, table 3, and supplementary files 11-13). No difference was found in the acceptability of non-benzodiazepine antispasmodics compared with control (relative risk 0.8, 95% confidence interval 0.6 to 1.1; 13 trials, 2834 participants; very low certainty evidence) (table 4 and supplementary file 14). Evidence ranging from moderate to low certainty showed no benefit of antispastic and benzodiazepine drugs compared with control for pain and disability at immediate (≤2 weeks) and short term (3-13 weeks) follow-up, except for reduction in disability associated with benzodiazepines at 3-13 weeks (mean difference −6.9, 95% confidence interval −12.1 to −1.7; 1 trial, 103 participants; moderate certainty evidence) (table 2, table 3, and supplementary files 11-13).
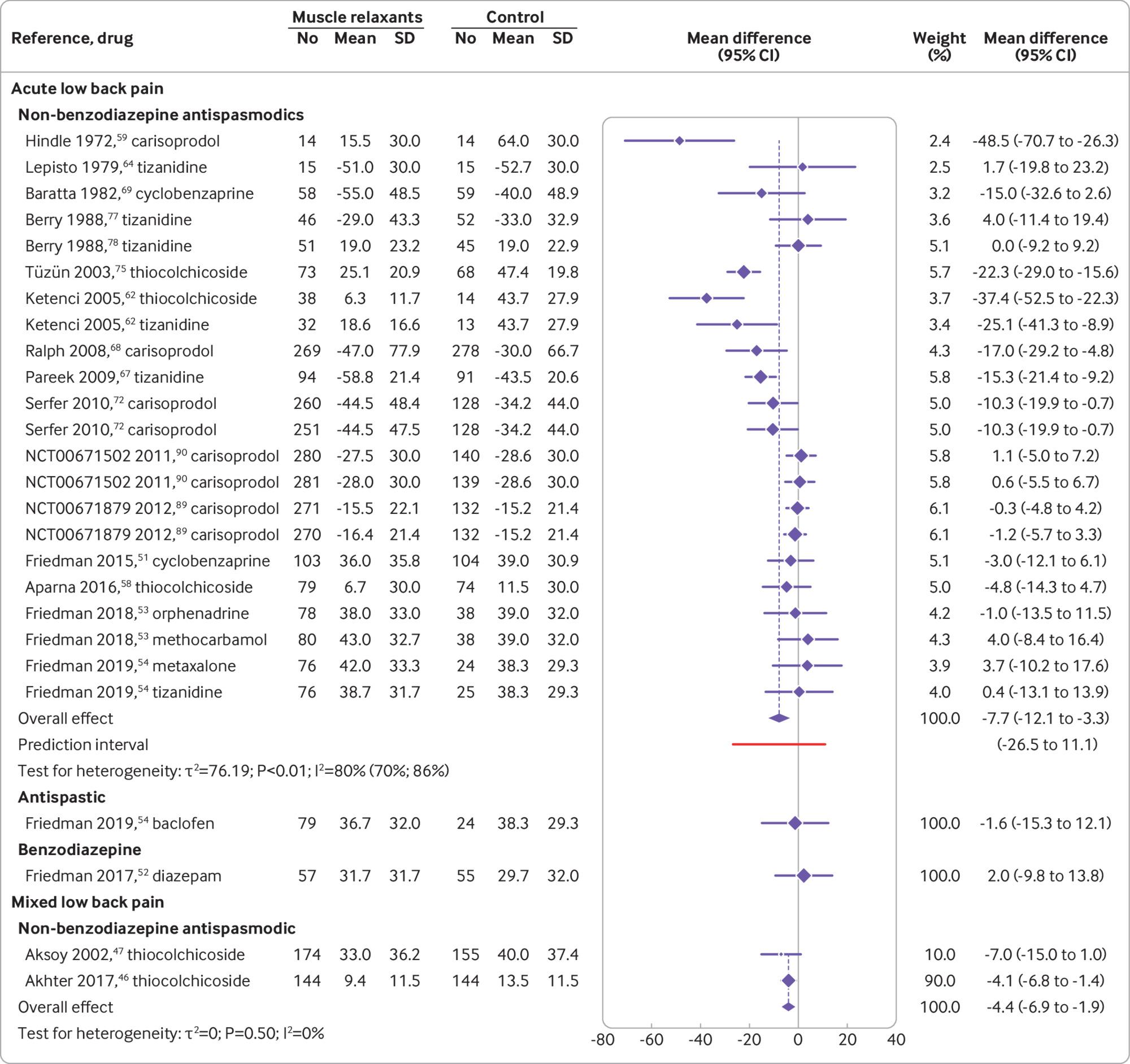
Effect of muscle relaxants compared with control on pain intensity (0-100 scale) at immediate term (≤2 weeks) post-randomisation for adults with low back pain. Negative values for mean differences indicate that effects favour muscle relaxants compared with control, whereas negative values for trial observations indicate change from baseline
{kind=link}
Summary of findings and certainty of evidence for low back pain in association with muscle relaxants
Summary of findings and certainty of evidence for disability from low back pain in association with muscle relaxants
Summary of findings and certainty of evidence for acceptability of muscle relaxants for low back pain
Subacute low back pain—One trial determined the efficacy of muscle relaxants on pain intensity at short term follow-up for subacute low back pain. Miscellaneous muscle relaxants (botulinum toxin) were not associated with a reduction in pain intensity compared with control (−19.0, −41.9 to 3.9; one trial, 28 participants; very low certainty evidence) (table 2 and supplementary file 11).
Chronic low back pain—Two trials (three comparisons) determined the efficacy of muscle relaxants on pain intensity at short term follow-up for chronic low back pain. Three trials (four comparisons) determined the acceptability of muscle relaxants for chronic low back pain. Evidence ranging from moderate to very low certainty showed no benefit compared with control for antispastic and miscellaneous muscle relaxants for pain, disability, and acceptability except for pain intensity at 3-13 weeks with miscellaneous muscle relaxants (eszoplicone) (−19.9, −31.5 to −8.3; 1 trial, 52 participants; moderate certainty evidence) (table 2, table 3, table 4, and supplementary files 11, 13, and 14).
Mixed low back pain—Two trials (two comparisons) determined the efficacy of muscle relaxants at immediate term follow-up and one trial at short term follow-up for mixed low back pain. Non-benzodiazepine antispasmodics were associated with a reduction in pain intensity at two weeks or less compared with control (−4.4, −6.9 to −1.9; 2 trials, 617 participants; low certainty) but not at 3-13 weeks (−5.8, −13.8 to 2.2; 1 trial, 329 participants; very low certainty evidence) (fig 2, table 2, and supplementary file 11). Non-benzodiazepine antispasmodics were associated with a reduction in disability at two weeks or less compared with control (−19.2, −27.7 to −10.7; 1 trial, 329 participants; low certainty evidence) (table 3 and supplementary file 12).
Safety
Acute low back pain—Twenty two trials (28 comparisons) determined the safety of muscle relaxants for acute low back pain. The type and reporting of adverse and serious adverse events varied across trials. Compared with control, non-benzodiazepine antispasmodics were associated with an increase in the risk of an adverse event (relative risk 1.6, 95% confidence interval 1.2 to 2.0; 16 trials, 3404 participants; low certainty evidence) but not a serious adverse event (2.3, 0.3 to 20.8; 2 trials, 830 participants; very low certainty evidence) (table 5 and supplementary files 15 and 16). Antispastic drugs were also associated with an increase in the risk of an adverse event (2.0, 1.1 to 3.8; 2 trials, 290 participants; moderate certainty evidence) whereas benzodiazepines were not (1.8, 0.9 to 3.6; 2 trials, 159 participants; low certainty evidence) (table 5 and supplementary file 15). Participants receiving antispastics were more likely to discontinue treatment owing to an adverse event (34.6, 2.1 to 568.0; 1 trial, 195 participants; very low certainty evidence) whereas participants receiving non-benzodiazepine antispasmodics were not (1.5, 0.6 to 3.5; 5 trials, 1641 participants; very low certainty evidence) (table 5 and supplementary file 17).
Summary of findings and certainty of evidence for safety of muscle relaxants for low back pain
Chronic low back pain—Two trials (two comparisons) determined the safety of muscle relaxants for chronic low back pain. Compared with control, no difference was found in the risk of experiencing an adverse event with miscellaneous muscle relaxants (1.5, 0.4 to 5.7; 2 trials, 95 participants; moderate certainty evidence) (table 5 and supplementary file 15).
Mixed low back pain—One trial determined the safety of muscle relaxants for mixed low back pain. Compared with control, no difference was found in the risk of experiencing an adverse event with non-benzodiazepine antispasmodics (1.6, 0.6 to 4.3; 1 trial, 329 participants; very low certainty evidence) (table 5 and supplementary file 15).
Subgroup and sensitivity analyses
Supplementary files 18-20 present detailed results for the subgroup, funnel plot, and sensitivity analyses, respectively. Owing to a lack of data, sensitivity analyses were only conducted for non-benzodiazepine antispasmodics for acute low back pain. The sensitivity analyses did not explain heterogeneity in the disability (≤2 weeks), acceptability, adverse events, and tolerability outcomes. When trials from clinical trial registries (mean difference −10.2, 95% confidence interval −15.6 to −4.7) or trials without a placebo comparator (−11, −17 to −5.1) were excluded, the estimated effect for pain intensity (≤2 weeks) changed to within the minimum clinically important difference. When excluding trials at high risk of bias, however, the effect decreased to zero (0.2, −4.9 to 5.4).
Discussion
We found very low certainty evidence that non-benzodiazepine antispasmodic drugs might reduce pain intensity at two weeks or less for patients with acute low back pain. This effect is small—less than 8 points on a 0–100 point scale—and does not meet common thresholds to be clinically meaningful. Non-benzodiazepine antispasmodics might have little to no effect on pain intensity at 3-13 weeks or on disability at all follow-up time points; however, the certainty of evidence ranged from moderate to very low. No trials evaluated the effect of muscle relaxants on long term outcomes. Low and very low certainty evidence showed that non-benzodiazepine antispasmodics might increase the risk of adverse events and might have little to no effect on treatment discontinuation, respectively. The number of trials investigating other muscle relaxants was small. The certainty of evidence was reduced because a large number of trials were at high risk of bias.
Strengths and weaknesses of this review
This systematic review was prospectively registered and reported in line with PRISMA.21 We included a broad scope of licensed muscle relaxants evaluated in randomised controlled trials as they provide the best evidence on the efficacy and safety of currently used muscle relaxants in clinical practice. We included findings from 49 trials of muscle relaxants for low back pain published up until 23 February 2021. To assess study level risk of bias we used the Cochrane risk of bias tool and published recommendations from the Cochrane Back and Neck Group34 and we evaluated the certainty of the evidence using the GRADE system.20 Finally, unlike with previous reviews,1795 we searched clinical trial registries for relevant trials.
Inadequate reporting and authors’ failure to respond to data requests meant some relevant trials were not included in each meta-analysis. We restricted the inclusion of studies based on publication language. Although we included trials published in English, Italian, Portuguese, Spanish, German, and Dutch, we could have missed some relevant trials. We relied on the definition of adverse and serious adverse events as reported from the included trials, therefore definitions might have varied between trials. We included trials in which participants received co-administered additional analgesics. Although most included trials compared drugs with placebo, the inclusion of other analgesics could have influenced the interpretation of findings. Finally, interpretation of the outcome acceptability has limitations because participants could discontinue treatment for any reason, including recovery.
Evidence update
Our review updates the evidence for use of muscle relaxants in adults with low back pain. For example, we included 31 trials (6505 participants) in the quantitative analysis, compared with 15 trials (3362 participants) in the most recent systematic review.17 Although the previous systematic reviews1795 and three clinical practice guidelines13 endorse non-benzodiazepine antispasmodics as an effective treatment for acute low back pain, we found considerable uncertainty in their clinical effectiveness and safety.
For this review we pooled data for all non-benzodiazepine antispasmodics according to the shared clinical utility in managing acute low back pain.8 The choice of muscle relaxant and frequency of prescription by a GP varies between countries.910 For example carisoprodol, commonly prescribed in the US,12 is no longer marketed in several Europeans countries96 or the UK97 because of an increased risk of misuse and dependency. We repeated the primary analyses after exclusion of trials that investigated carisoprodol and found that effects were comparable.
Meaning of the study
Although the observed effect of non-benzodiazepine antispasmodics in reducing pain compared with control at two weeks or less was statistically significant, the magnitude of the effect was too small to be considered clinically important. The upper limits of the confidence interval do not, however, exclude a clinically meaningful effect on pain intensity. The modest overall effect is reported at group level, which could still mean that some, but not all, individuals gain a worthwhile benefit.98
We identified important heterogeneity in the effect of non-benzodiazepine antispasmodics on pain, with the prediction interval spanning −26.5 to 11.1. Heterogeneity might have increased because of the inclusion of trials reporting unusually large effects, such as that of Hindle et al published in 197259 (−48.5, −70.7 to −26.3), where the placebo comparison showed no change from baseline, which is atypical of the clinical course of recovery for patients with acute low back pain.99 The subgroup and sensitivity analyses were unable to explain the heterogeneity observed in the pooled effect for pain. Restricting the analysis to a comparison of non-benzodiazepine antispasmodics with placebo showed a statistically significant effect greater than the threshold for minimally clinical important difference. As the removal of high risk of bias trials reduced the effect to zero, however, we advise caution when interpreting these findings.
Implications for clinical practice and policy
International clinical practice guidelines provide conflicting recommendations for the use of muscle relaxants11; of 15 clinical practice guidelines, six recommend muscle relaxants to manage low back pain, five do not recommend them, and four do not offer a recommendation.13 Our review shows uncertainty of evidence for the efficacy and safety of muscle relaxants. Although non-benzodiazepine antispasmodics might reduce pain intensity at two weeks or less for acute low back pain, the effect is unlikely to be considered clinically important. In addition, non-benzodiazepine antispasmodics could increase the risk of an adverse event being reported (commonly, dizziness, drowsiness, headache, and nausea100), but might have little to no effect on treatment discontinuation, suggesting the treatment and increased risk of adverse events are acceptable. The low to very low certainty of evidence does not, however, allow any firm recommendations. We would encourage clinicians to discuss this uncertainty in the efficacy and safety of muscle relaxants with patients, sharing information about the possibility for a worthwhile benefit in pain reduction but increased risk of experiencing a non-serious adverse event, to allow them to make informed treatment decisions.
Unanswered questions and future research
Large, definitive, placebo controlled trials are urgently needed to evaluate the efficacy and safety of muscle relaxants. New trials should follow the core outcome set for non-specific low back pain101 and the recommendations of the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials,102 to improve the pooling of results and comparability between trials. Future trials should also endeavour to adhere to methodological safeguards to reduce bias and transparently report results following the Consolidated Standards of Reporting Trials statement.103
Although muscle relaxants are typically prescribed for short term use, the effects of long term use are not known. High quality data are required to evaluate the efficacy and safety of long term use. This is particularly important when considering that the risk of dependency and misuse associated with muscle relaxants has been observed from indirect evidence.95100
Conclusions
This systematic review found very low certainty evidence that non-benzodiazepine antispasmodics for the treatment of acute low back pain might provide a small and not clinically meaningful improvement in pain intensity at two weeks or less. The risk of adverse events but not serious adverse events might be increased with use of non-benzodiazepine antispasmodics, although the evidence ranges from low to very low certainty. Large, high quality, placebo controlled trials are urgently needed to resolve uncertainties about the efficacy and safety of muscle relaxants for low back pain.
What is already known on this topic
Muscle relaxants are the third most frequently prescribed drugs for low back pain
Clinical practice guidelines provide conflicting recommendations for the use of muscle relaxants to treat low back pain
What this study adds
Very low certainty evidence shows that non-benzodiazepine antispasmodics might offer a small, non-clinically important reduction in pain intensity at two weeks or less for acute low back pain
Low and very low certainty evidence shows non-benzodiazepine antispasmodics might increase the risk of adverse events and might have little to no effect on treatment discontinuation compared with control, respectively
Large, definitive, placebo controlled trials are urgently needed to resolve uncertainties about the efficacy and safety of muscle relaxants
Ethics statements
Ethical approval
Ethical approval: Not required.
Data availability statement
Data sharing: The dataset used and analysed during this study and the accompanying code are available from the corresponding author on reasonable request.
Footnotes
Contributors: TF, MKB, and JHM conceived the study. TF, MKB, MAW, MCF, SMS, SMG, RD, and JHM contributed to the study design and protocol development. TF conducted the search. AGC, TF, MKB, MDJ, MAW, MCF, RRNR, and HBL selected the studies, extracted data, and did the quality appraisal. AGC and MAW analysed the data. AGC, MAW, and JHM had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. AGC wrote the first draft of the manuscript. All authors provided substantive feedback on the manuscript and have read and approved the final version. AGC is the guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. AGC is supported by the University of New South Wales (UNSW) Prince of Wales Clinical School postgraduate research scholarship and a Neuroscience Research Australia (NeuRA) PhD candidature supplementary scholarship. MKB is supported by a NeuRA PhD candidature scholarship and supplementary scholarship and was additionally funded during this work by an Australian government research training programme scholarship and a UNSW research excellence award. MAW is supported by a university postgraduate award and School of Medical Sciences top-up scholarship from UNSW, and a postgraduate scholarship from the National Health and Medical Research Council of Australia. MCF is supported by an Australian medical research future fund grant (GNTID1170205). HBL is supported by an Australian government postgraduate award. RRNR is supported by UNSW School of Medical Sciences postgraduate research scholarship and a NeuRA PhD candidature supplementary scholarship. SMS receives salary support from the National Health and Medical Research Council of Australia (#1105040). SMG is supported by the Rebecca L Cooper Medical Research Foundation. JHM receives project funding support from the National Health and Medical Research Council and the Medical Research Future Fund of Australia.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
The lead author (AGC) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: We will disseminate our findings to patient organisations and through traditional media and social media outlets.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.