Prevalence, Related Factors, and Levels of Burnout Syndrome Among Nurses Working in Gynecology and Obstetrics Services: A Systematic Review and Meta-Analysis


 ,
,  , and
, and
Abstract
:1. Introduction
2. Material and Methods
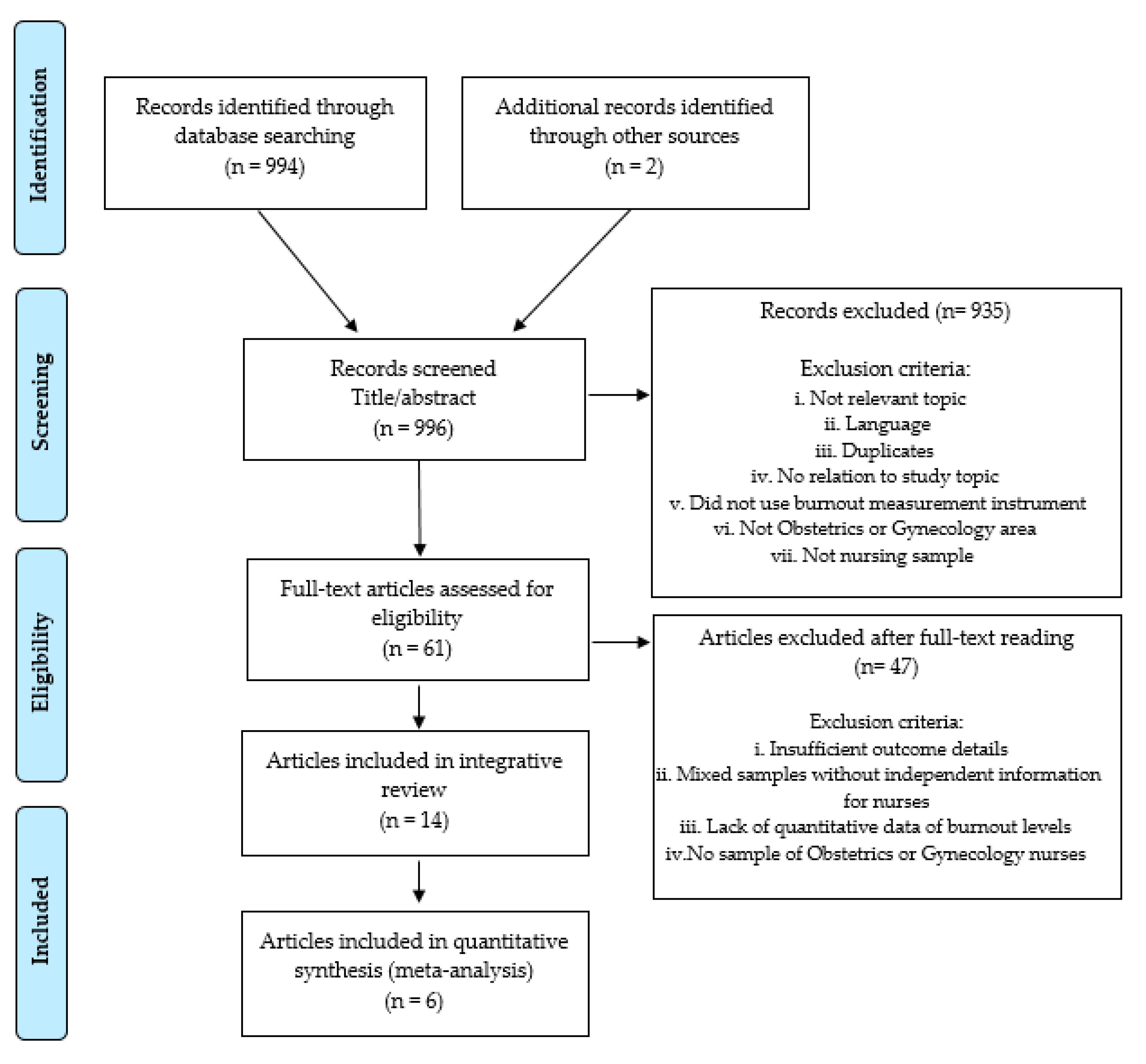
2.1. Search Strategy
2.2. Study Selection, Critical Review, and Level of Evidence
2.3. Data Coding
2.4. Data Analysis
3. Results
3.1. Dimensions of Burnout Syndrome in the Area of Gynecology and Obstetrics
3.2. Related Factors for Burnout in Gynecology and Obstetrics Services
3.3. Levels of Burnout in Comparison with Nurses Working in Other Hospital Services
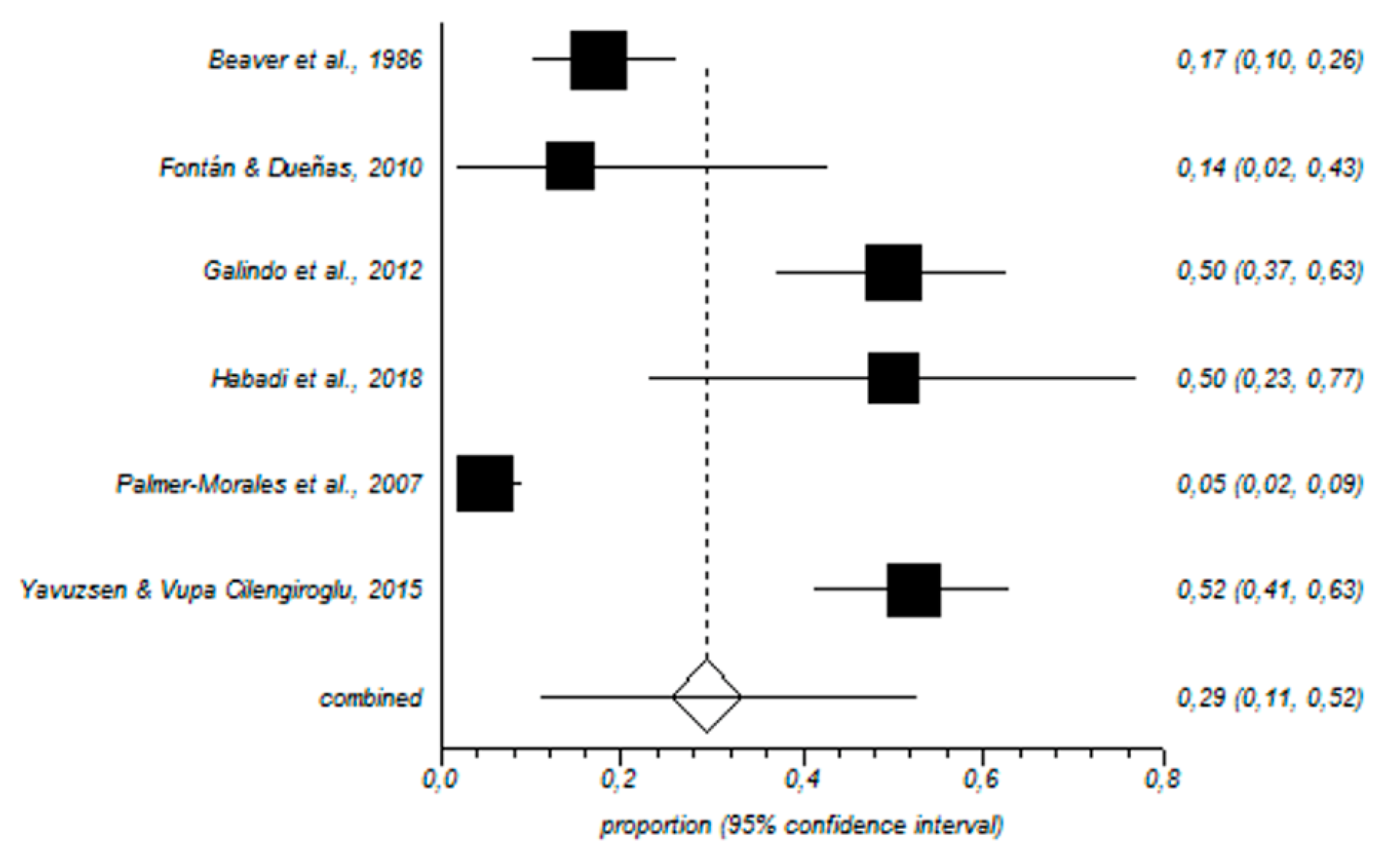
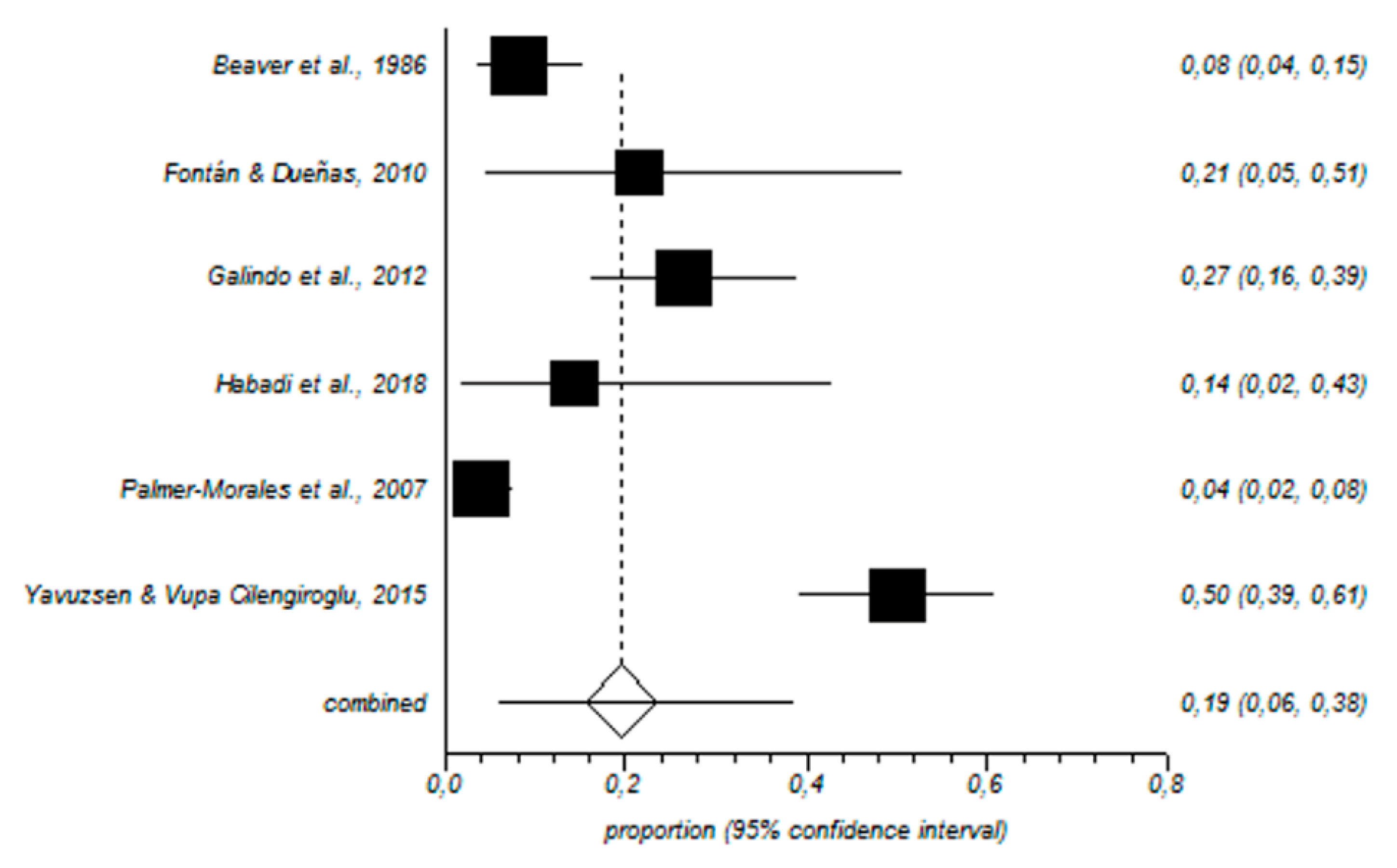
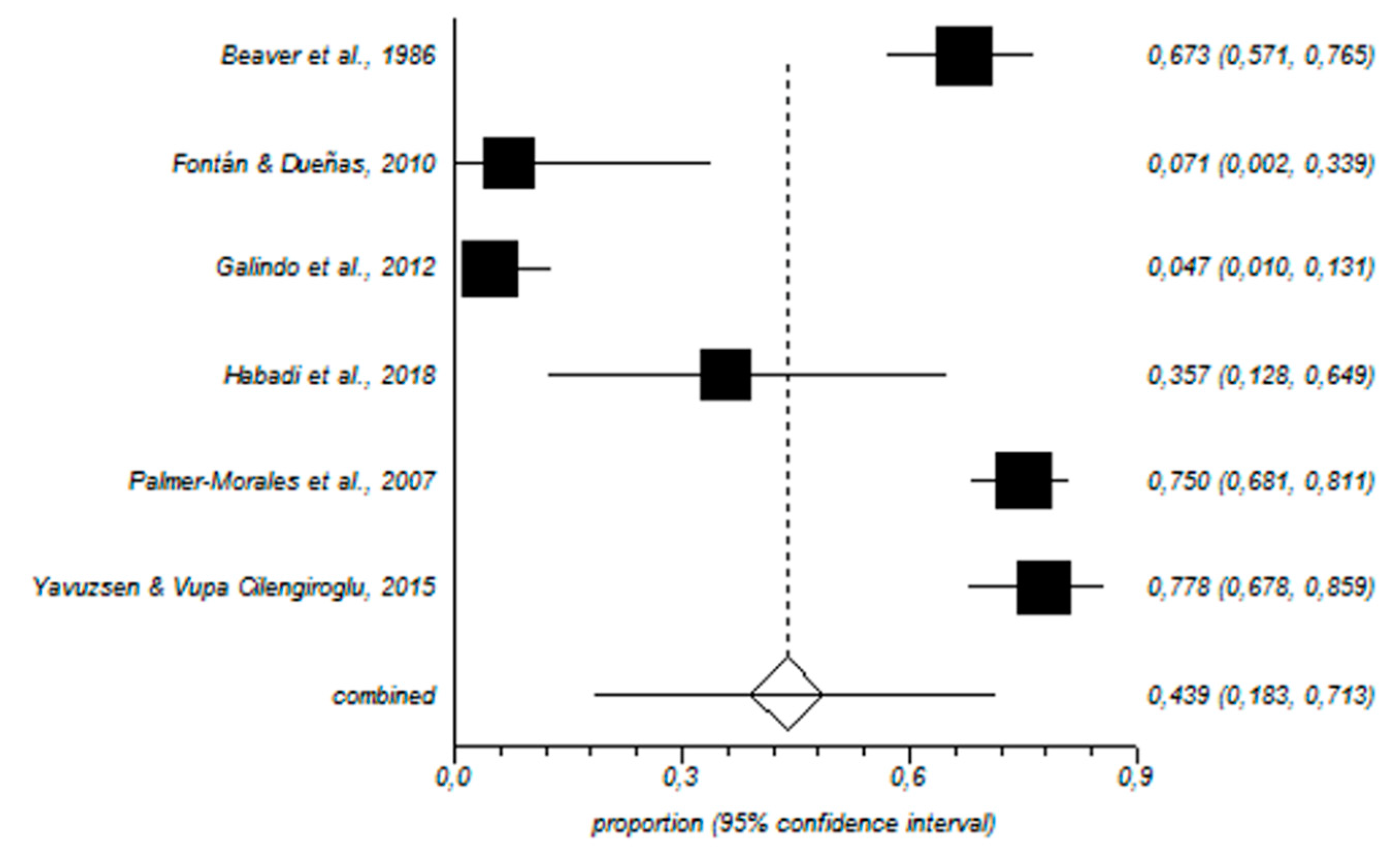
3.4. Results of the Meta-Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Salyers, M.P.; Bonfils, K.A.; Luther, L.; Firmin, R.L.; White, D.A.; Adams, E.L.; Rollins, A.L. The relationship between professional burnout and quality and safety in healthcare: A meta-analysis. J. Gen. Intern. Med. 2017, 32, 475–482. [Google Scholar] [CrossRef] [PubMed]
- McVicar, A. Scoping the common antecedents of job stress and job satisfaction for nurses (2000–2013) using the job demands resources model of stress. J. Nurs. Manag. 2016, 24, E112–E136. [Google Scholar] [CrossRef] [PubMed]
- Ruitenburg, M.M.; Frings-Dresen, M.H.; Sluiter, J.K. The prevalence of common mental disorders among hospital physicians and their association with self-reported work ability: A cross-sectional study. BMC Health Serv. Res. 2012, 12, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Hämmig, O. Explaining burnout and the intention to leave the profession among health professionals-A cross-sectional study in a hospital setting in Switzerland. Bmc Health Serv. Res. 2018, 18, 785. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P.; Schaufeli, W.B.; Schwab, R.L. MBI: The Maslach Burnout Inventory Manual; Consulting Psychologists Press: Palo Alto, CA, USA, 1996. [Google Scholar]
- Cañadas-De la Fuente, G.A.; Ortega, E.; Ramírez-Baena, L.; De la Fuente-Solana, E.I.; Vargas, C.; Gómez-Urquiza, J.L. Gender, marital Status, and children as risk factors for burnout in nurses: A Meta-Analytic Study. Int. J. Environ. Res. Public Health 2018, 15, 2102. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Urquiza, J.L.; Vargas, C.; De la Fuente, E.I.; Fernández-Castillo, R.; Cañadas-De la Fuente, G.A. Age as a risk factor for burnout syndrome in nursing professionals: A meta-analytic study. Res. Nurs. Health 2017, 40, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Emold, C.; Schneider, N.; Meller, I.; Yagil, Y. Communication skills, working environment and burnout among oncology nurses. Eur. J. Oncol. Nurs. 2011, 15, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos Alves, D.F.; da Silva, D.; de Brito Guirardello, E. Nursing practice environment, job outcomes and safety climate: A structural equation modelling analysis. J. Nurs. Manag. 2017, 25, 46–55. [Google Scholar] [CrossRef]
- Guo, Y.F.; Plummer, V.; Lam, L.; Wang, Y.; Cross, W.; Zhang, J.P. The effects of resilience and turnover intention on nurses burnout: Findings from a comparative cross-sectional study. J. Clin. Nurs. 2019, 28, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.F.; Chiang, H.Y.; Kuo, H.T. Relationship between authentic leadership and nurses intent to leave: The mediating role of work environment and burnout. J. Nurs. Manag. 2019, 27, 52–65. [Google Scholar] [CrossRef] [PubMed]
- Scanlan, J.N.; Still, M. Relationships between burnout, turnover intention, job satisfaction, job demands and job resources for mental health personnel in an Australian mental health service. BMC Health Serv. Res. 2019, 19, 62. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi, O.; Azizkhani, R.; Basravi, M. Correlation between workplace and occupational burnout syndrome in nurses. Adv. Biomed. Res. 2014, 3, 44. [Google Scholar] [CrossRef]
- Cañadas-De la Fuente, G.A.; Vargas, C.; San Luis, C.; García, I.; Cañadas, G.R.; De La Fuente, E.I. Risk factors and prevalence of burnout syndrome in the nursing profession. Int. J. Nurs. Stud. 2015, 52, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Urquiza, J.L.; De la Fuente-Solana, E.I.; Albendín-García, L.; Vargas-Pecino, C.; Ortega-Campos, E.M.; Cañadas-De la Fuente, G.A. Prevalence of burnout syndrome in emergency nurses: A Meta-Analysis. Crit. Care Nurse 2017, 37, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Monsalve-Reyes, C.S.; San Luis-Costas, C.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo, R.; Cañadas-De la Fuente, G.A. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Baena, L.; Ortega-Campos, E.; Gómez-Urquiza, J.L.; Cañadas-De la Fuente, G.R.; De la Fuente-Solana, E.I.; Cañadas-De la Fuente, G.A. A multicentre study of burnout prevalence and related psychological variables in medical area hospital nurses. J. Clin. Med. 2019, 8, 92. [Google Scholar] [CrossRef]
- Noonan, M.; Jomeen, J.; Galvin, R.; Doody, O. Survey of midwives perinatal mental health knowledge, confidence, attitudes and learning needs. Women Birth 2018, 31, e358–e366. [Google Scholar] [CrossRef] [PubMed]
- Wahlberg, A.; Högberg, U.; Emmelin, M. The erratic pathway to regaining a professional self-image after an obstetric work-related trauma: A grounded theory study. Int. J. Nurs. Stud. 2019, 89, 53–61. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Ciapponi, A. Critical appraisal guide of observational studies in epidemiology (first part). Evidencia 2010, 13, 135–140. [Google Scholar]
- Howick, J.; Chalmers, I.; Glasziou, P.; Greenhalg, T.; Heneghan, C.; Liberati, A.; Moschetti, I.; Phillips, B.; Thornton, H. The Oxford 2011 Levels of Evidence. 2011. Available online: https://www.cebm.net/2016/05/ocebm-levels-of-evidence (accessed on 10 April 2019).
- Beaver, R.C.; Sharp, E.S.; Cotsonis, G.A. Burnout experienced by nurse midwives. J. Nurs. Midwifery 1986, 31, 3–15. [Google Scholar] [CrossRef]
- Fontán Atalaya, I.M.; Dueñas Díez, J.L. Burnout syndrome in an obstetrics and gynaecology management unit. Rev. Calid. Asist. 2010, 25, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Galindo, R.H.; Feliciano, K.V.; Lima, R.A.; de Souza, A.I. Burnout syndrome among general hospital nurses in Recife. Rev. Esc. Enferm. USP 2012, 46, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Habadi, A.I.; Alfaer, S.S.; Shilli, R.H.; Habadi, M.I.; Suliman, S.M.; Al-Aslany, S.J.; Habadi, M.I. The prevalence of burnout syndrome among nursing staff working at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, 2017. Divers. Equal. Health Care 2018, 15, 122–126. [Google Scholar] [CrossRef]
- Higashiguchi, K.; Morikawa, Y.; Miura, K.; Nishijo, M.; Tabata, M.; Ishizaki, M.; Nakagawa, H. Burnout and related factors among hospital Nurses. J. Occup. Health 1999, 41, 215–224. [Google Scholar] [CrossRef]
- Liu, W.; Zhao, S.; Shi, L.; Zhang, Z.; Liu, X.; Li, L.; Duan, X.; Li, G.; Lou, F.; Jia, X.; et al. Workplace violence, job satisfaction, burnout, perceived organisational support and their effects on turnover intention among Chinese nurses in tertiary hospitals: A cross-sectional study. BMJ Open 2018, 8, e019525. [Google Scholar] [CrossRef]
- Mizuno, M.; Kinefuchi, E.; Kimura, R.; Tsuda, A. Professional quality of life of Japanese nurses/midwives providing abortion/childbirth care. Nurs. Ethics 2013, 20, 539–550. [Google Scholar] [CrossRef]
- Naz, S.; Hashmi, A.M.; Asif, A. Burnout and quality of life in nurses of a tertiary care hospital in Pakistan. J. Pak. Med. Assoc. 2016, 66, 532–536. [Google Scholar]
- Nguyen, H.T.T.; Kitaoka, K.; Sukigara, M.; Thai, A.L. Burnout study of clinical nurses in Vietnam: Development of job burnout model based on Leiter and Maslachs Theory. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2018, 12, 42–49. [Google Scholar] [CrossRef]
- Palmer-Morales, Y.; Prince-Vélez, R.; Searcy-Bernal, R.; Compean-Saucedo, B. Prevalence of burnout syndrome in nurses in 2 Mexican hospitals. Enferm. Clin. 2007, 17, 256–260. [Google Scholar] [CrossRef]
- Sun, W.Y.; Ling, G.P.; Chen, P.; Shan, L. Burnout among nurses in the peoples Republic of China. Int. J. Occup. Environ. Health 1996, 2, 274–279. [Google Scholar] [CrossRef]
- Teffo, M.E.; Levin, J.; Rispel, L.C. Compassion satisfaction, burnout and secondary traumatic stress among termination of pregnancy providers in two South African provinces. J. Obstet. Gynaecol. Res. 2018, 44, 1202–1210. [Google Scholar] [CrossRef]
- Yao, Y.; Zhao, S.; Gao, X.; An, Z.; Wang, S.; Li, H.; Li, Y.; Gao, L.; Lu, L.; Dong, Z. General self-efficacy modifies the effect of stress on burnout in nurses with different personality types. BMC Health Serv. Res. 2018, 18, 667. [Google Scholar] [CrossRef]
- Yavuzşen, H.T.; Vupa Çilengiroğlu, O. Burnout in physicians and nurses working in Obstetrics/Gynecology clinics in Turkey. Turkiye Klinikleri J. Gynecol. Obst. 2015, 25, 160–167. [Google Scholar] [CrossRef]
- Molina-Praena, J.; Ramírez-Baena, L.; Gómez-Urquiza, J.L.; Cañadas, G.R.; De la Fuente, E.I.; Cañadas-De la Fuente, G.A. Levels of burnout and risk factors in medical area nurses: A meta-analytic study. Int. J. Environ. Res. Public Health 2018, 15, 2800. [Google Scholar] [CrossRef]
- Pradas-Hernández, L.; Ariza, T.; Gómez-Urquiza, J.L.; Albendín-García, L.; De la Fuente, E.I.; Cañadas-De la Fuente, G.A. Prevalence of burnout in paediatric nurses: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195039. [Google Scholar] [CrossRef]
- Moradi, Y.; Baradaran, H.R.; Yazdandoost, M.; Atrak, S.; Kashanian, M. Prevalence of burnout in residents of obstetrics and gynecology: A systematic review and meta-analysis. Med. J. Islam. Repub. Iran 2015, 29, 235. [Google Scholar]
- Thorsen, V.C.; Tharp, A.L.; Meguid, T. High rates of burnout among maternal health staff at a referral hospital in Malawi: A cross-sectional study. BMC Nurs. 2011, 10, 9. [Google Scholar] [CrossRef]
- Govardhan, L.M.; Pinelli, V.; Schnatz, P.F. Burnout, depression and job satisfaction in obstetrics and gynecology residents. Conn. Med. 2012, 76, 389–395. [Google Scholar]
- Gabbe, S.G.; Melville, J.; Mandel, L.; Walker, E. Burnout in chair of obstetrics and gynecology: Diagnosis, treatment, and prevention. Am. J. Obstet. Gynecol. 2002, 186, 601–612. [Google Scholar] [CrossRef]
- De la Fuente-Solana, E.I.; Cañadas, G.R.; Ramirez-Baena, L.; Gómez-Urquiza, J.L.; Ariza, T.; Cañadas-De la Fuente, G.A. An explanatory model of potential changes in burnout diagnosis according to personality factors in oncology nurses. Int. J. Environ. Res. Public Health 2019, 16, 312. [Google Scholar] [CrossRef]
- Iorga, M.; Socolov, V.; Muraru, D.; Dirtu, C.; Soponaru, C.; Ilea, C.; Socolov, D.M. Factors influencing burnout syndrome in obstetrics and gynecology physicians. Biomed. Res. Int. 2017, 2017, 1–10. [Google Scholar] [CrossRef]
- Kavurmacı, M.; Cantekin, I.; Tan, M. Burnout levels of hemodialysis nurses. Ren. Fail. 2014, 36, 1038–1042. [Google Scholar] [CrossRef] [Green Version]
- Flinkman, M.; Isopahkala-Bouret, U.; Salanterä, S. Young registered nurses intention to leave the profession and professional turnover in early career: A qualitative case study. ISRN Nurs. 2013, 2013, 1–12. [Google Scholar] [CrossRef]
- França, S.P.; Martino, M.F.; Aniceto, E.V.; Silva, L.L. Preditores da síndrome de burnout emenfermeiros de serviços de urgencia pré-hospitalar. Acta Paul. Enferm. 2012, 25, 68–73. [Google Scholar] [CrossRef]
- Hildingsson, I.; Westlund, K.; Wiklund, I. Burnout in Swedish midwives. Sex. Reprod. Health 2013, 4, 87–91. [Google Scholar] [CrossRef]
- Rudman, A.; Gustavsson, P.; Hultell, D. A prospective study of nurses intentions to leave the profession during their first five years of practice in Sweden. Int. J. Nurs. Stud. 2014, 51, 612–662. [Google Scholar] [CrossRef]
- McAuliffe, E.; Daly, M.; Kamwendo, F.; Masanja, H.; Sidat, M.; de Pinho, H. The critical role of supervision in retaining staff in obstetric services: A three country study. PLoS ONE 2013, 8, e58415. [Google Scholar] [CrossRef]
- Hellyar, M.; Madani, C.; Yeaman, S.; O′Connor, K.; Kerr, K.M.; Davidson, J.E. Case study investigation decreases burnout while improving interprofessional teamwork, nurse satisfaction, and patient safety. Crit Care Nurs Q. 2019, 42, 96–105. [Google Scholar] [CrossRef]
- Heinen, M.M.; van Achterberg, T.; Schwendimann, R.; Zander, B.; Matthews, A.; Kózka, M.; Ensio, A.; Sjetne, I.S.; Moreno Casbas, T.; Ball, J.; et al. Nurses intention to leave their profession: A cross sectional observational study in 10 European countries. Int. J. Nurs. Stud. 2013, 50, 174–184. [Google Scholar] [CrossRef]
- Moloney, W.; Boxall, P.; Parsons, M.; Cheung, G. Factors predicting registered nurses intentions to leave their organization and profession: A job demands-resources framework. J. Adv. Nurs. 2018, 74, 864–875. [Google Scholar] [CrossRef]
- Winkel, A.F.; Robinson, A.; Jones, A.A.; Squires, A.P. Physician resilience: A grounded theory study of obstetrics and gynaecology residents. Med. Educ. 2019, 53, 184–194. [Google Scholar] [CrossRef]
- Kozhimannil, K.B.; Hung, P.; Henning-Smith, C.; Casey, M.M.; Prasad, S. Association between loss of hospital-based obstetric services and birth outcomes in rural counties in the United States. JAMA 2018, 319, 1239–1247. [Google Scholar] [CrossRef]
- Nowrouzi, B.; Lightfoot, N.; Carter, L.; Larivière, M.; Rukholm, E.; Schinke, R.; Belanger-Gardner, D. The relationship between quality of work life and location of cross-training among obstetric nurses in urban northeastern Ontario, Canada: A population-based cross sectional study. Int. J. Occup. Med. Environ. Health 2015, 28, 571–586. [Google Scholar] [CrossRef] [Green Version]
- Labrague, L.J.; McEnroe-Petitte, D.M.; Tsaras, K. Predictors and outcomes of nurse professional autonomy: A cross-sectional study. Int. J. Nurs. Pract. 2019, 25, 12711. [Google Scholar] [CrossRef]
- Bermudez-Tamayo, C.; Fernández Ruiz, E.; Pastor Moreno, G.; Maroto-Navarro, G.; Garcia-Mochon, L.; Perez-Ramos, F.J.; Caño-Aguilar, A.; Velez, M.D.P. Barriers and enablers in the implementation of a program to reduce cesarean deliveries. Reprod. Health 2017, 14, 106. [Google Scholar] [CrossRef] [Green Version]
- Cañadas-De la Fuente, G.A.; Albendín-García, L.; De la Fuente, E.I.; San Luis, C.; Gómez-Urquiza, J.L.; Cañadas, G.R. Síndrome de burnout en profesionales de enfermería que realizan jornada física complementaria en servicios de cuidados críticos y urgencias. Rev. Esp. Salud Pública 2016, 90, e1–e9. [Google Scholar]
- Campanelli, S. The ties that bind-nurses, mothers, and antepartum care. Nurs. Womens Health 2019, 23, 181–182. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; Daryl, B.O. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Olsen, E.; Bjaalid, G.; Mikkelsen, A. Work climate and the mediating role of workplace bullying related to job performance, job satisfaction, and work ability: A study among hospital nurses. J. Adv. Nurs. 2017, 73, 2709–2719. [Google Scholar] [CrossRef]
- Prentice, T.M.; Gillam, L.; Davis, P.G.; Janvier, A. Always a burden? Healthcare providers perspectives on moral distress. Arch. Dis. Child. Fetal Neonatal. Ed. 2018, 103, F441–F445. [Google Scholar] [CrossRef]
- Elmir, R.; Pangas, J.; Dahlen, H.; Schmied, V. A meta-ethnographic synthesis of midwives and nurses experiences of adverse labour and birth events. J. Clin. Nurs. 2017, 26, 4184–4200. [Google Scholar] [CrossRef]
- Gong, Y.; Han, T.; Yin, X.; Yang, G.; Zhuang, R.; Chen, Y.; Lu, Z. Prevalence of depressive symptoms and work-related risk factors among nurses in public hospitals in southern China: A cross-sectional study. Sci. Rep. 2014, 4, 7109. [Google Scholar] [CrossRef]
- Beck, C.T.; Eaton, C.M.; Gable, R.K. Vicarious posttraumatic growth in labor and delivery nurses. J. Obstet. Gynecol. Neonatal. Nurs. 2016, 45, 801–812. [Google Scholar] [CrossRef]
- Hamama-Raz, Y.; Walker, R.; Palgi, Y.; Mashiach, R.; Lee-Ovadia, K.; Manny, A.; Ben-Ezra, M. Comorbidity of post-traumatic stress symptoms and depressive symptoms among obstetric nurses with perinatal death exposure. Isr. J. Psychiatry Relat. Sci. 2016, 53, 58–62. [Google Scholar]
- Ben-Ezra, M.; Palgi, Y.; Walker, R.; Many, A.; Hamam-Raz, Y. The impact of perinatal death on obstetrics nurses: A longitudinal and cross-sectional examination. J. Perinat. Med. 2014, 42, 75–81. [Google Scholar] [CrossRef]
- Blackmore, E.R.; Côté-Arsenault, D.; Tang, W.; Glover, V.; Evans, J.; Golding, J.; O’Connor, T.G. Previous prenatal loss as a predictor of perinatal depression and anxiety. Br. J. Psychiatry 2011, 198, 373–378. [Google Scholar] [CrossRef] [Green Version]
- Suplee, P.D.; Bingham, D.; Kleppel, L. Nurses knowledge and teaching of possible postpartum complications. MCN Am. J. Matern. Child Nurs. 2017, 42, 338–344. [Google Scholar] [CrossRef]
- Wang, J.; Cui, Y.; He, L.; Xu, X.; Yuan, Z.; Jin, X.; Li, Z. Work-Related musculoskeletal disorders and risk factors among Chinese medical staff of obstetrics and gynecology. Int. J. Environ. Res. Public Health 2017, 14, 562. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2014, 13, CD002892. [Google Scholar] [CrossRef]
- Craigie, M.; Slatyer, S.; Hegney, D.; Osseiran-Moisson, R.; Gentry, E.; Davis, S.; Dolan, T.; Rees, C. A pilot evaluation of a Mindful Self-care and Resiliency (MSCR) intervention for nurses. Mindfulness 2016, 7, 764–774. [Google Scholar] [CrossRef]
- Lupo, F.N.; Arnaboldi, P.; Santoro, L.; D’Anna, E.; Beltrami, C.; Mazzoleni, E.M.; Veronesi, P.; Maggioni, A.; Didier, F. The effects of a multimodal training program on burnout syndrome in gynecologic oncology nurses and on the multidisciplinary psychosocial care of gynecologic cancer patients: An Italian experience. Palliat. Support Care 2013, 11, 199–203. [Google Scholar] [CrossRef]
- Cocchiara, R.A.; Peruzzo, M.; Mannocci, A.; Ottolenghi, L.; Villari, P.; Polimeni, A.; Guerra, F.; La Torre, G. The use of yoga to manage stress and burnout in healthcare workers: A systematic review. J. Clin. Med. 2019, 8, 284. [Google Scholar] [CrossRef]
- Babbar, S.; Renner, K.; Williams, K. Addressing obstetrics and gynecology trainee burnout using a yoga-based wellness initiative during dedicated education time. Obstet. Gynecol. 2019, 133, 994–1001. [Google Scholar] [CrossRef]
- Salvarani, V.; Rampoldi, G.; Ardenghi, S.; Bani, M.; Blasi, P.; Ausili, D.; Di Mauro, S.; Strepparava, M.G. Protecting emergency room nurses from burnout: The role of dispositional mindfulness, emotion regulation and empathy. J. Nurs. Manag. 2019, 27, 765–774. [Google Scholar] [CrossRef]
- Montanari, K.M.; Bowe, C.; Chesak, S.S.; Cutshall, S.M. Assessing the feasibility of a pilot intervention to reduce stress and burnout. J. Holist. Nurs. 2019, 37, 175–188. [Google Scholar] [CrossRef]
- Mealer, M.; Conrad, D.; Evans, J.; Jooste, K.; Solyntjes, J.; Rothbaum, B.; Moss, M. Feasibility and acceptability of a resilience training program for intensive care unit nurses. Am. J. Crit. Care 2014, 23, e97–e105. [Google Scholar] [CrossRef]
- Mackenzie, C.S.; Poulin, P.A.; Seidman-Carlson, R. A brief mindfulness-based stress reduction intervention for nurses and nurse aides. Appl. Nurs. Res. 2006, 19, 105–109. [Google Scholar] [CrossRef]
- Leiter, M.P.; Maslach, C. Latent burnout profiles: A new approach to understanding the burnout experience. Burn. Res. 2016, 3, 89–100. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country | Study Design | Sample (Gender and Mean Age) | Burnout Instrument (Reliability, Cronbach’s α) | M (SD)/Percentage | Main Results | OCEBM GR/LE | ||
|---|---|---|---|---|---|---|---|---|
| EE | D | PA | ||||||
| Beaver et al., 1986, USA [25] | Cross-sectional | N = 98 O&G nurses 96.9% Female Age = 30–39: 55.2% | MBI (EE = 0.82, D = 0.60, PA = 0.80) | Low: 58.2% Moderate: 25.5% High: 16.3% | Low: 73.5% Moderate: 18.4% High: 8.2% | Low: 67.3% Moderate: 20.4% High: 12.2% | EE and D are negatively related to age and experience, and positively to the number of births and weekly work hours. | 2c/B |
| Fontán and Dueñas, 2010, Spain [26] | Cross-sectional | N = 14 O&G nurses 78.57% Female Age = 46 | MBI | 12.2 (10.6) High: 14.2% | 5.0 (5.5) High: 21.4% | 45.1 (7.1) Low 7.1% | Highest levels are found in professionals who work more than 48 hours per week. Lower level of burnout at older age. | 2c/B |
| Galindo et al., 2012, Brazil [27] | Cross-sectional | N = 64 O&G nurses 92.1% Female Age = 29 | MBI (EE = 0.86, D = 0.69, PA = 0.76) | Low: 20.6% Moderate: 30.2% High: 49.2% | Low:14.3% Moderate: 58.7% High: 27% | Low: 4.8% Moderate: 11.1% High: 84.1% | Burnout correlates negatively with salary, experience, and age. A good organization of the service reduces the risk of burnout syndrome. | 2c/B |
| Habadi et al., 2018, Saudi Arabia [28] | Cross-sectional | N = 14 O&G nurses | MBI | High: 50% | High: 14.28% | Low: 28.57% | O&G area is considered one of the lowest prevalences of burnout. | 2c/B |
| Higashiguchi et al., 1999, Japan [29] | Cross-sectional | N = 28 O&G nurses | MBI (Japanese Version) | 3.48 (1.29) | 1.67 (0.72) | 3.64 (1.10) | Low prevalence of burnout with high levels of PA in O&G unit nurses. | 2c/B |
| Liu et al., 2018, China [30] | Cross-sectional | N = 93 O&G nurses | MBI (EE = 0.83, D = 0.83, PA = 0.81) | - | - | - | Low burnout score in O&G nurses (M: 6.19, SD: 2.71). Positive correlation between burnout and rotating shifts (r = 0.444). | 2c/B |
| Mizuno et al., 2013, Japan [31] | Cross-sectional | N = 169 O&G nurses Age = 42.4 | ProQOL FEWS | Subscale | High emotional burden on nurses in this area. Burnout correlates with the number of abortions, increasing stress, and reducing job satisfaction. | 2c/B | ||
| Compassion satisfaction = 33 (6.9) Burnout = 26.75 (5.4) Compassion fatigue = 20.75 (5.65) | ||||||||
| Naz et al., 2016, Pakistan [32] | Cross-sectional | N = 28 O&G nurses | MBI | 55.8 (6.7) | 29.5 (3.4) | 21.8 (4.9) | O&G service nurses have a higher burnout score compared to other services, such as medicine, surgery, neurology, or psychiatry. | 2c/B |
| Nguyen et al., 2018, Korea [33] | Cross-sectional | N = 122 O&G nurses | MBI (Vietnamese version) (EE = 0.89, D = 0.77, PA = 0.80) | 2.98 (1.00) | 2.72 (0.88) | 3.77 (0.77) | Higher EE scores in pediatric and medical area. Higher scores of D and lower in PA in pediatric and O&G area. | 2c/B |
| Palmer-Morales et al., 2007, Mexico [34] | Cross-sectional | N=184 O&G nurses | MBI | Low: 78.8% Moderate: 16.3% High: 4.9% | Low: 91.85% Moderate: 4.35% High: 3.8% | Low: 75% Moderate: 14.7% High: 10.3% | There is no correlation between marital status and number of children and years of work experience with risk of burnout. | 2c/B |
| Sun et al., 1996, China [35] | Cross-sectional | N = 273 O&G nurses | MBI (EE = 0.87, D = 0.81, PA = 0.84) | 25.30 (2.99) | 12.93 (1.75) | 29.90 (2.65) | O&G units present high burnout. The main factor is stress and urgency related to the life of the mother or child. | 2c/B |
| Teffo et al., 2018, South Africa [36] | Cross-sectional | N = 73 O&G nurses | PRoQOL | Subscale | An adequate work environment increases motivation and job satisfaction. Burnout is related to years of experience. | 2c/B | ||
| Compassion satisfaction = 41 (5.7) Burnout = 33 (4.1) Secondary traumatic stress = 24 (7) | ||||||||
| Yao et al., 2018, China [37] | Cross-sectional | N = 95 O&G nurses | MBI | 12.0 (5.9) | 7.0 (4.7) | 10.9 (8.9) | Emergencies, mental health, and pediatrics are the areas with the highest burnout score. O&G area presents the lowest score in burnout. | 2c/B |
| Yavuzşen and Vupa Çilengiroğlu, 2015, Turkey [38] | Cross-sectional | N = 90 O&G nurses 100% Female Age = 35.49 | MBI (EE = 0.90, D = 0.77, PA = 0.74) | 27.59 (7.27) High: 52% | 10.00 (3.59) High: 50% | 30.06 (4.41) Low 78% | D correlates negatively with age. Age, being a woman, and being single are considered related factors. | 2c/B |
| Study | Sample Size (n) | High EE (%) | High D (%) | Low PA (%) |
|---|---|---|---|---|
| Beaver et al., 1986 [25] | 98 | 16.3 | 8.2 | 67.3 |
| Fontán & Dueñas, 2010 [26] | 14 | 14.2 | 21.4 | 7.1 |
| Galindo et al., 2012 [27] | 64 | 49.2 | 27 | 4.8 |
| Habadi et al., 2018 [28] | 14 | 50 | 14.28 | 28.57 |
| Palmer-Morales et al., 2007 [34] | 184 | 4.9 | 3.8 | 75 |
| Yavuzşen & Vupa Çilengiroğlu, 2015 [38] | 90 | 52 | 50 | 78 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De la Fuente-Solana, E.I.; Suleiman-Martos, N.; Pradas-Hernández, L.; Gomez-Urquiza, J.L.; Cañadas-De la Fuente, G.A.; Albendín-García, L. Prevalence, Related Factors, and Levels of Burnout Syndrome Among Nurses Working in Gynecology and Obstetrics Services: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2585. https://doi.org/10.3390/ijerph16142585
De la Fuente-Solana EI, Suleiman-Martos N, Pradas-Hernández L, Gomez-Urquiza JL, Cañadas-De la Fuente GA, Albendín-García L. Prevalence, Related Factors, and Levels of Burnout Syndrome Among Nurses Working in Gynecology and Obstetrics Services: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(14):2585. https://doi.org/10.3390/ijerph16142585
Chicago/Turabian StyleDe la Fuente-Solana, Emilia I., Nora Suleiman-Martos, Laura Pradas-Hernández, Jose L. Gomez-Urquiza, Guillermo A. Cañadas-De la Fuente, and Luis Albendín-García. 2019. "Prevalence, Related Factors, and Levels of Burnout Syndrome Among Nurses Working in Gynecology and Obstetrics Services: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 14: 2585. https://doi.org/10.3390/ijerph16142585