Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
About A Rare Case of Small Neuroendocrine
Carcinoma of the Mandible at the University
Hospital of Casablanca in Morocco
Ismael Coulibaly1, Hanane Rida1, Tarik Chékrine1, Zineb Bouchbika1, Nadia. Benchakroun1, Hassan Jouhadi1,
Nezha. Tawfiq1, Souha Sahraoui1
1
Mohamed VI Center for the Treatment of cancers, CHU Ibn Rochd, Hospital Districts, 20360 Casablanca, Morocco
Abstract :- Neuroendocrine tumors (NETs) arise from II. CLINICAL CASE
neuroendocrine cells and are mostly observed in the
gastrointestinal tract, pancreas, and lungs. NETs in the A 67-year-old Moroccan man, chronic smoker at 15
oral and maxillofacial region are extremely rare. We pack-years, weaned 10 years ago. He is known hypertensive
report a case of a 67-year-old man with an NET in the with cardiac arrhythmia controlled under treatment. He has a
mandible. The patient did not show any symptoms history of eye surgery for cataract in 2009. This patient was
except for remarkable jugular swelling. The lesion seen in consultation for a swelling of the right cheek
appeared as a radiolucent honeycomb abnormality with evolving for 08 months and gradually increasing in size
bone destruction on panoramic radiography. The becoming painful, the starting point of which would be the
histopathologic diagnosis following a biopsy was NET. right mandibular angle. On clinical examination, the patient
Contrast-enhanced computed tomography (CT), 18F- was in good general condition with a WHO Performance
fluorodeoxyglucose positron emission computed Status of 1. There was a voluminous swelling on the right
tomography (18F-FDG PET/CT), showed tumor mass of cheek of about 20 cm in long axis, painful, taking the
the soft parts of the right mandible with bone lysis ascending branch of the mandible with infiltration in endo -
without lymph node, visceral or bone hypermetabolism . buccal (Picture 1). Mouth opening was limited and there was
He had three chemotherapy cures with good clinical and no peripheral clinical lymphadenopathy.
radiological response followed by concomitant radio
chemotherapy 60Gy.The evolution was marked by a A cervico-facial scan was performed showing tumor
febrile grade IV aplasia leading to the death of the mass under and latero mandibular right coming into contact
patient. Neuroendocrine carcinomas of mandible are with the right parotid and encompassing the submaxillary
unusual. Their prognosis is overall bleak. The responsible for mandibular lysis (Image 3)
morphological characteristics, the clinical aspects and
the therapeutic management of these tumors are A biopsy of the mass was performed. The histological
comparable to the neuroendocrine tumors of the lung. study shows a malignant proliferation of undifferentiated
round cells of medium size with an indistinct scanty
Keywords :- Neuroendocrine Small Cell Carcinoma, cytoplasm and a hyperchromic, irregular, sometimes
Mandible, Radiotherapy, Chemotherapy, Surgery. strongly nucleolated nucleus. Immunohistochemical study
showed tumor cells with intense and diffuse synaptophysin
I. INTRODUCTION positivity, but negative for chromogranin A, cytokeratin, CD
20, CD 3, CD 99, desmin and myogenin with a Ki 67 at
Neuroendocrine tumors arise from neuroendocrine 60%.
cells and are mainly seen in the gastrointestinal tract,
pancreas and lungs [1]. Neuroendocrine cells of the oral Positron emission tomography with 18 FDG coupled
mucosa are an underestimated component of the with CT scan showed a hyper metabolic process of the soft
neuroendocrine system whose biological roles are elusive in tissues encompassing the right mandible with bone lysis
the oral cavity [2]. Neuroendocrine carcinoma is a tumor extending submandibularly and ascending along the
that occurs in different places, especially the lungs and the ascending branch of the mandible with a max SUV at 10.22
larynx. The oral cavity is a very rare location for primary for a max liver SUV at 2.2 (Image 5). There was no lymph
neuroendocrine carcinomas [3]. These tumors also have a node, visceral or bone hypermetabolism.
very unfavorable prognosis. The diagnosis is often made at
an advanced stage which further darkens its prognosis. Due Based on these findings, a diagnosis of poorly
to their rarity, there is no standard of care. The treatment is differentiated small cell neuroendocrine carcinoma of the
generally based on the data already known in the right locally advanced gingiva was made. The patient
management of pulmonary localization. However, it is received 3 courses of neoadjuvant chemotherapy based on
necessary to be familiar with the different therapeutic Etoposide + Cisplatin. He developed non-febrile Grade 2
modalities for better management. We report a case of neutropenia after the second course. Post-chemotherapy
neuroendocrine carcinoma of the gum. evaluation by cervico-facial CT scan noted a 90% regression
in size of the mass (Image 4). For surgeons, a surgical
IJISRT22SEP1109 www.ijisrt.com 1963
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
intervention would be very dilapidating with a Diagnosis is based on pathological examination. On
mandibulectomy. We therefore decided on concomitant histological examination, the diagnosis of the
radio-chemotherapy with dose reduction: association of neuroendocrine nature of these tumors is suggested by
homolateral locoregional irradiation at a dose of 60 Gray in morphology and confirmed after an immunohistochemistry
classic fractionation of 30 sessions and two sessions of study. The morphological aspect is similar to what is
etoposide 100 mg and cisplatin 20 mg chemotherapy on D1 observed in the lung: neuroendocrine morphology with a
and at D21. After 15 radiotherapy sessions, the patient high mitotic and necrotic power. The cells are large, with
presented with grade 3 mucositis plus non-febrile grade 4 moderate to abundant cytoplasm [20]. In terms of
neutropenia, which led us to stop radiotherapy and immunohistochemistry, neuroendocrine carcinomas are
hospitalize him. The patient unfortunately died in an array of defined by the presence of neuroendocrine markers,
multi-visceral failure. essentially chromogranin A, synaptophysin, neuron-specific
enolase (NSE) and CD56 [20]. However, the expression of
III. DISCUSSION neuroendocrine markers is inconstant and the absence of
expression of one of these markers does not exclude the
A neuroendocrine tumor is an epithelial tumor whose diagnosis of neuroendocrine carcinoma. In the 04 cases of
cells present structural, phenotypic and functional neuroendocrine carcinoma of the gingiva published in the
characteristics reminiscent of those of normal endocrine literature that we reported, synaptophysin was always
cells secreting peptide hormones [2]. They constitute a expressed whereas chromogranin was positive in only 3
heterogeneous group of tumors arising from cells of the patients [3; 17; 18; 19]. In our observation, only
diffuse neuroendocrine system [4]. They differ in their synaptophysin is expressed. However, to retain the diagnosis
location, embryological origin, degree of differentiation, of a neuroendocrine carcinoma of the gum with certainty,
biological behavior, functional activity and size but share the presence of another primary site must be excluded. In
common morphological, immunohistochemical and the literature, the clinical manifestations are not always
structural characteristics [5]. These are rare tumors but can described, but in most localizations of the oral cavity, we
be found in most locations. There are several classifications find a painful swelling as a reason for consultation [3], as in
of neuroendocrine tumors depending on the primary our case. The general condition is most often preserved at
location. On the head and neck, they are classified as typical the time of diagnosis.
carcinoid, atypical carcinoid, small cell neuroendocrine
carcinoma which can be well, moderately or poorly Computed tomography has been used in the arsenal of
differentiated [6; 7]. the paraclinical assessment in several studies. The place of
PET-FDG is not clearly defined, it is mainly used to search
The predilection site of neuroendocrine carcinomas is for clinically non-noisy secondary localizations
the lung and the digestive tract. But other rare locations are
encountered in the literature, in this case gynecological [8; Therapeutically, there is no therapeutic standard given
9; 10], head and neck [11; 12], bladder [13] and breast [14; the rarity of neuroendocrine carcinomas of the gums.
15]. In terms of ENT and stomatology, the frequent location Radical surgery and adjuvant chemotherapy using cisplatin
is the larynx, gingival neuroendocrine carcinoma is and etoposide seem to be good options for localized forms
exceptional [2]. In an analysis of the National Cancer Center [21]. The rechemoth dieterapie for carcinomaatsmall cells of
database in 2017 in the United States, out of 1042 patients lung origin, which includes genotecisplatin andetoposide is
with small cell carcinoma of the head and neck, only 9% had most often used [11]. In case of non-metastatic disease,
an oral location [12]. Small cell neuroendocrine carcinoma chemotherapy can be used in neoadjuvant or adjuvant
is frequently encountered in the elderly with a history of treatment to reduce tumor burden and reduce the risk of
smoking, as is the case in our patient [16]. ENT and dental distant metastasis. In a series published by Pointer et al in
neuroendocrine carcinomas are very aggressive and have an 2017, 61% of patients had received chemotherapy and
unfavorable prognosis with lymph node, locoregional and radiotherapy combined. Concomitant radiochemotherapy
distant involvement [12; 17]. Small cell forms are rare in the was the most frequent treatment in patients with early and
oral cavity and very few are localized to the gumline. HAS locally advanced disease [12]. Although surgery has an
To our knowledge, we find in the literature a case localized important role in local control, the Pointer et al series
at the level of the retromolar trigone described by Benning showed that adding surgery to radiotherapy and
et al [18], a case reported by Mochizuki Y et al [17] on the chemotherapy in patients with locally advanced disease does
upper gum but combined with squamous cell carcinoma. not did not result in improved survival compared to patients
Zeng M et al [19] reported a case on the lower gingiva and a treated with combined radiotherapy and chemotherapy [12].
case on the lower anterior gingiva was reported by Wu The case reported by Benning et al [18] had been treated
Zhang B. et al in 2014 in a 25-year-old woman with chemotherapy only and the evolution was marked by a
[3].Epidemiologically, the sex ratio is 6/1 for locoregional recurrence and the patient died of his disease
neuroendocrine carcinomas of the oral cavity and 11/1 for 30 months after diagnosis. Overall survival for all patients
localizations of the oral mucosa. Most patients are over 50 with small cell carcinoma of the head and neck was 20.3
years old [2]. months in the National Cancer study [12]. In light of these
data from the literature which highlight the role of systemic
treatment in this disease, neoadjuvant chemotherapy is
recommended before any local treatment in locally
IJISRT22SEP1109 www.ijisrt.com 1964
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
advanced disease. Faced with a locally advanced disease, the IV. CONCLUSION
prognosis is poor from the outset, the trimodal treatment
consisting of chemotherapy, surgery and radiotherapy, Although neuroendocrine carcinomas are well
which is the ideal combination, hardly improves survival described in certain locations, particularly the lungs, they
[12]. In our case the patient responded well to neoadjuvant remain a poorly understood entity, especially in the oral
chemotherapy, the observed toxicity could be related to the location. Due to the lack of knowledge about this type of
concomitant chemotherapy. tumor coupled with their non-specific clinical behavior, the
disease often reaches an advanced stage before the diagnosis
is made, making cure impossible. We have reported a case
of rare neuroendocrine carcinoma occurring in the gingiva.
He had a reserved prognosis from the outset with local
invasion. We consider that for locally advanced forms that
cannot be resected from the outset:
APPENDICES
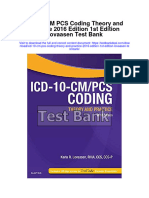
Picture 1 Photo at the First Day in Consult. Picture 2 Photo After 3 Courses of Chemotherapy
Picture 3 Axial Slice on Diagnostic CT Picture 4 CT Slice After Chemo
IJISRT22SEP1109 www.ijisrt.com 1965
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Picture 5 PET Image of Diagnostic
Table 1 Distribution Of Cases Reported In The Literature
Authors Age/Sex Size (Cm) Extension Treatment Survival In Months
Wu Zhang B et 25/F 1.5x2 localized Wide surgery only 13 months progression-free
al survival
38/F 2x3 localized Surgery + Radiotherapy 08 months progression-free
survival
Mochizuki Y et 62/F 2x0.8x0.6 localized Surgery with 23 months progression-free
al [17] maxillectomy only survival
Benning et al 63/M Unspecified localized Chemotherapy + Local recurrence at 08 months
[18] Radiotherapy 60 Gray Distant metastasis at 20
months
Death at 24 months
Zeng M et al 73/M 2.8x2x1.4 localized Large surgery and 14 months progression-free
[19] partial mandibulectomy survival
+ chemo
REFRENCES [6]. Said-Al-Naief, N., Sciandra, K., & Gnepp, DR
(2013). Moderately Differentiated Neuroendocrine
[1]. Sugawara, C., Takahashi, A., Kawano, F., Kudoh, T., Carcinoma (Atypical Carcinoid) of the Parotid Gland:
Yamada, A., Ishimaru, N.,… Miyamoto, Y. (2015). Report of Three Cases with Contemporary Review of
Neuroendocrine tumor in the mandible: a case report Salivary Neuroendocrine Carcinomas. Head and
with imaging and histopathological findings. Oral Neck Pathology, 7(3), 295–303. doi:10.1007/s12105-
Surgery, Oral Medicine, Oral Pathology and Oral 013-0431-6
Radiology, 119(1), e41–e48. doi:10.1016 /j.oooo. [7]. Barnes, L., Eveson, JW, Reichart, P., Sidransky, D.
2014.09.024 World Health Organization Classification of
[2]. Mohammed, F. (2010). Neuroendocrine cells and Tumours, Volume 9. Pathology and Genetics of Head
associated malignancies of the oral mucosa: a review. and Neck Tumours. IARC Press Lyon 2005 430 p
Journal of Oral Pathology & Medicine, 39(2), 121– [8]. Dundr P, Fischerová D, Povy´ sˇil C, Cibula D.
127. doi:10.1111/j.1600-0714.2009.00834.x Primary pure large-cell neuroendocrine carcinoma of
[3]. Wu, B.-Z., Gao, Y., & Yi, B. (2014). Primary the ovary. Pathol Res Practice 2008;204:133–7.
Neuroendocrine Carcinoma in Oral Cavity: Two Case [9]. Gonzalez-Bosquet E, Gaba L, Saco MA2, Gil-Ibañez
Reports and Review of the Literature. Journal of Oral B, Fuster P, Glickman A3, Torne A3 Metastatic
and Maxillofacial Surgery, 72(3), 633–644. Large Cell Neuroendocrine Carcinoma of the
doi:10.1016/j.joms.2013.08.020 Endometrium: A Case Report and Literature Review.
[4]. A. Oudidi, H. Hachimi, MN El Alami Obstet Gynecol Res 2018; 1 (4): 094-100 DOI:
[Neuroendocrine carcinoma of parotid gland]. Ann 10.26502/ogr015
Endocrinol. 2016 Sept; 67(4):360-3 [10]. Erhan Y, Dickmen Y, Yucebilgin MS, Zekioglu O,
[5]. M. SCHLUMBERGER, E. BAUDIN Mgoyi L, Terek MC. Large cell neuroendocrine
[Neuroendocrine tumors]. Ann Endocrinol. 1997 ; 58 carcinoma of the uterine corpus metastatic to brain
(2): 95-9 and lung: case report and review of the literature. Eur
J Gynaecol Oncol 2004;25:109–12.
IJISRT22SEP1109 www.ijisrt.com 1966
Volume 7, Issue 9, September – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[11]. Renner, G. (2007). Small Cell Carcinoma of the Head
and Neck: A Review. Seminars in Oncology, 34(1),
3–14. doi:10.1053/j.seminoncol.2006.10.024
[12]. Pointer, KB, Ko, HC, Brower, JV, Witek, ME,
Kimple, RJ, Lloyd, RV, … Baschnagel, AM (2017).
Small cell carcinoma of the head and neck: An
analysis of the National Cancer Database. Oral
Oncology, 69, 92–98.
doi:10.1016/j.oraloncology.2017.04.009
[13]. Safini, F., Jouhadi, H., Marnissi, F., Bouchbika, Z.,
Benchakroun, N., Tawfiq, N., … Benider, A. (2018).
Small cell neuroendocrine carcinoma of the bladder:
about five cases and review of the literature.
Cancer/Radiotherapy.
doi:10.1016/j.canrad.2017.11.014
[14]. Safini, F., Bouchbika, Z., Bennani, Z., Belkheiri, S.,
Attar, HE, Benchakroun, N.,… Benider, A. (2016).
Primary large cell neuroendocrine carcinoma of the
breast: a rare tumor in men. Pan African Medical
Journal, 25. doi:10.11604/pamj.2016.25.205.10366
[15]. Bourhaleb, Z., Uri, N., Haddad, H., Azzouzi, S.,
Zamiati, S., Benchakroun, N., … Benider, A. (2009).
Large cell neuroendocrine carcinoma of the breast:
about a case and review of the literature.
Cancer/Radiotherapy, 13(8), 775–777.
doi:10.1016/j.canrad.2009.06.021
[16]. Salama, AR, Jham, BC, Papadimitriou, JC, &
Scheper, MA (2009). Metastatic neuroendocrine
carcinomas to the head and neck: report of 4 cases
and review of the literature. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology, and
Endodontology, 108(2), 242–247.
doi:10.1016/j.tripleo.2009.03.030
[17]. Mochizuki, Y., Omura, K., Sakamoto, K., Nakanishi,
S., Satoh, K., Marukawa, E., & Yamaguchi, A.
(2010). A case of primary combined neuroendocrine
carcinoma with squamous cell carcinoma in the upper
gingiva. Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology, and Endodontology,
109(4), e34–e39. doi:10.1016/j.tripleo.2009.12.018
[18]. Benning TL, Vollmer RT, Crain BJ, Shelburne JD.
neuroendocrine carcinoma of the oral cavity. mod
Pathol 1990; 3:631-4.
[19]. ZENG, M., YANG, S.-D., ZHANG, J.-L., & CHEN,
X.-M. (2015). Primary small cell neuroendocrine
carcinoma of the oral cavity: A case report and
review of the literature. Oncology Letters, 10(2),
887–890. doi:10.3892/ol.2015.3298
[20]. Saint Andre JP, Valo I, Guyetant S. Pathological
anatomy of neuroendocrine tumors. Mem Acad Chir
(Paris) 2003;2:47–52.
[21]. Lin, Y.-C., Wu, H.-P., & Tzeng, J.-E. (2005). Small-
cell undifferentiated carcinoma of the submandibular
gland: an extremely rare extrapulmonary site.
American Journal of Otolaryngology, 26(1), 60–63.
doi:10.1016/j.amjoto.2004.06.013
IJISRT22SEP1109 www.ijisrt.com 1967
You might also like
- Decrease in Visual Acuity As The Ini.3tial Clinical Presentation of Lung Adenocarcinoma A Case ReportDocument6 pagesDecrease in Visual Acuity As The Ini.3tial Clinical Presentation of Lung Adenocarcinoma A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rare Case of Metastatic Nodular Adrenal Ganglioneuroblastoma To Bone in A Young Female at Ibn Rochd University Hospital of Casablanca in MoroccoDocument7 pagesRare Case of Metastatic Nodular Adrenal Ganglioneuroblastoma To Bone in A Young Female at Ibn Rochd University Hospital of Casablanca in MoroccoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Small Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportDocument4 pagesSmall Cell Neuroendocrine Carcinoma of Bartholin's Gland: A Case ReportAfrican Journal of Medicine and Pharma ResearchNo ratings yet
- Follicular Dendritic Cell Sarcoma of The Tonssilar About A CaseDocument4 pagesFollicular Dendritic Cell Sarcoma of The Tonssilar About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Rhabdoid Tumor of The Kidney in Children A Rare Case ReportDocument3 pagesRhabdoid Tumor of The Kidney in Children A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportDocument4 pagesAn Atypical Esthesioneuroblastoma of The Sphenoid Sinus A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Proptosis UnilateralDocument5 pagesProptosis UnilateralCarlos NiveloNo ratings yet
- Odontogenickeratocyst Clinically Mimicking Osteomyelitis - A Rare Case ReportDocument4 pagesOdontogenickeratocyst Clinically Mimicking Osteomyelitis - A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Inflammatory Myofibroblastic TumourDocument4 pagesInflammatory Myofibroblastic TumourThiruNo ratings yet
- Unusual Cases of Carcinoma of Palatine TonsilDocument5 pagesUnusual Cases of Carcinoma of Palatine TonsilPridho GaziansyahNo ratings yet
- Adult Orbital Rhabdomyosarcoma Case ReportDocument3 pagesAdult Orbital Rhabdomyosarcoma Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NocardiaDocument6 pagesNocardiadocalsultanNo ratings yet
- Nasal Pyramid Skin's Adenosquamous Carcinoma A Rare Case ReportDocument3 pagesNasal Pyramid Skin's Adenosquamous Carcinoma A Rare Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Gingia MandibularaDocument4 pagesGingia MandibularamadalinaNo ratings yet
- Olfactory Groove MeningiomaDocument16 pagesOlfactory Groove Meningiomaclaudio RivasNo ratings yet
- Nasogpangeal AdenoidDocument6 pagesNasogpangeal AdenoidSanggiani Diah AuliaNo ratings yet
- Tuberculosis of The Nasal Cavities About Four CasesDocument5 pagesTuberculosis of The Nasal Cavities About Four CasesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Synchronous Squamous Cell Carcinoma of The Lip and Nasopharyngeal Carcinoma - A Rare Case Report.Document4 pagesSynchronous Squamous Cell Carcinoma of The Lip and Nasopharyngeal Carcinoma - A Rare Case Report.International Journal of Innovative Science and Research Technology100% (1)
- Jurnal Mata 1Document6 pagesJurnal Mata 1Elison J PanggaloNo ratings yet
- Fast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseFrom EverandFast Facts: Blastic Plasmacytoid Dendritic Cell Neoplasm: Shedding light on a rare diseaseNo ratings yet
- Pi Is 0278239103007407Document5 pagesPi Is 0278239103007407tengoplatita2008No ratings yet
- DIAGNOSIS AND MANAGEMENT OF CONJUNCTIVAL MELANOMADocument14 pagesDIAGNOSIS AND MANAGEMENT OF CONJUNCTIVAL MELANOMADyerik LilingNo ratings yet
- An Infrequent Secondary Location of Renal Carcinoma About A CaseDocument7 pagesAn Infrequent Secondary Location of Renal Carcinoma About A CaseInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Bulbo-Medullary Ependymoma in An Adult: Case ReportDocument6 pagesBulbo-Medullary Ependymoma in An Adult: Case ReportIJAR JOURNALNo ratings yet
- Confirmed Tuberculous Brain Miliary in an Immunocompetent Patient: A Case ReportDocument3 pagesConfirmed Tuberculous Brain Miliary in an Immunocompetent Patient: A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Epithelial-Myoepithelial Carcinoma Arising in The Accessory Parotid Gland A Case ReportDocument4 pagesEpithelial-Myoepithelial Carcinoma Arising in The Accessory Parotid Gland A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ba So CelularDocument13 pagesBa So CelularMihaela BubulacNo ratings yet
- F0605yDocument6 pagesF0605ySetiaty PandiaNo ratings yet
- Hannoun 2021Document4 pagesHannoun 2021mahaaNo ratings yet
- An Uncommon Cancer of Parotid Squamous Cell HistologyDocument3 pagesAn Uncommon Cancer of Parotid Squamous Cell HistologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1 s2.0 S2352512623003600 MainDocument3 pages1 s2.0 S2352512623003600 MainKikin RizkynnisaNo ratings yet
- Brainstem CysticercoseDocument4 pagesBrainstem CysticercoseDr. R. SANKAR CITNo ratings yet
- Rare Case of Zosteriform Metastases from Hard Palate CancerDocument4 pagesRare Case of Zosteriform Metastases from Hard Palate CancerShiva PNo ratings yet
- Tonsil TumorDocument4 pagesTonsil TumorafrisiammyNo ratings yet
- 6324-Article Text-21760-1-10-20210620Document3 pages6324-Article Text-21760-1-10-20210620Fritzienico BaskoroNo ratings yet
- Malignant Pheochromocytoma - A Diagnostic and Therapeutic DilemmaDocument5 pagesMalignant Pheochromocytoma - A Diagnostic and Therapeutic DilemmaJad DegheiliNo ratings yet
- Large CystDocument4 pagesLarge CystKin DacikinukNo ratings yet
- Severe Fungal Cervicofacial Cellulitis From Otogenic Mucuromycosis Origin A Case ReportDocument4 pagesSevere Fungal Cervicofacial Cellulitis From Otogenic Mucuromycosis Origin A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Actinomycotic Brain Abscess: Case ReportDocument3 pagesActinomycotic Brain Abscess: Case ReportIqbal AbdillahNo ratings yet
- Merkel Cell Carcinoma: A Case ReportDocument6 pagesMerkel Cell Carcinoma: A Case ReportIJAR JOURNALNo ratings yet
- 3504-Article Text-11497-1-10-20200318Document3 pages3504-Article Text-11497-1-10-20200318Ade Puji AstutiNo ratings yet
- Bmhim 23 80 1 063-068Document6 pagesBmhim 23 80 1 063-068Karina CamachoNo ratings yet
- Medicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic LaryngitisDocument4 pagesMedicine: An Unusual Extranodal Natural Killer/t-Cell Lymphoma Presenting As Chronic Laryngitisnurul atika havizNo ratings yet
- PAAF en WilmsDocument10 pagesPAAF en WilmsMarcela Di VincenzoNo ratings yet
- Dermatofibrosarcoma Protuberans: Retrospective Single Center Analysis Over 16 YearsDocument3 pagesDermatofibrosarcoma Protuberans: Retrospective Single Center Analysis Over 16 YearsdrelvNo ratings yet
- Orbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportDocument4 pagesOrbital Metastasis of A Pediatric Nasopharyngeal Carcinoma A Rare Case ReportInternational Journal of Innovative Science and Research Technology100% (1)
- Mucoepidermoid Carcinomaof The External Auditory Canal (Eac)Document4 pagesMucoepidermoid Carcinomaof The External Auditory Canal (Eac)IJAR JOURNALNo ratings yet
- ContentsDocument3 pagesContentsNaim CalilNo ratings yet
- Peripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewDocument4 pagesPeripheral Primitive Neuro-Ectodermal Tumor of The Pleura About A Rare Caser, With Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CarcinomaDocument5 pagesCarcinomaLori SimmonsNo ratings yet
- Adenoid Cystic Carcinoma of Hard Palate: A Case ReportDocument5 pagesAdenoid Cystic Carcinoma of Hard Palate: A Case ReportHemant GuptaNo ratings yet
- 1 Neurosurgery Cases and ReviewsDocument5 pages1 Neurosurgery Cases and ReviewsintodoieblissNo ratings yet
- Cerebellopontine Angle Epidermoid CYST: Case ReportDocument3 pagesCerebellopontine Angle Epidermoid CYST: Case ReportTamajyoti GhoshNo ratings yet
- Ijoo D 18 00333Document18 pagesIjoo D 18 00333DrKunal KaradeNo ratings yet
- Rare Cases in ENTDocument5 pagesRare Cases in ENTshadia sameerNo ratings yet
- Two Cases of Subungual Melanoma of The Thumb in SituDocument5 pagesTwo Cases of Subungual Melanoma of The Thumb in SituIJAR JOURNALNo ratings yet
- Extra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalDocument5 pagesExtra Renal Rhabdoid Tumor in An Adult Presentin 2024 International JournalRonald QuezadaNo ratings yet
- Maxillary Chondrosarcoma Case Report and Literature ReviewDocument5 pagesMaxillary Chondrosarcoma Case Report and Literature ReviewMulki MaajidNo ratings yet
- 5725-Article Text-20053-1-10-20210320Document3 pages5725-Article Text-20053-1-10-20210320Rafael BagusNo ratings yet
- medi-101-e29739Document4 pagesmedi-101-e29739MARSELLA MICHELLE ERIKA SUMANGKUTNo ratings yet
- Visual Water: An Integration of App and Web to Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web to Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in a Stenosed Artery under the Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in a Sten. Art. Under the Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis on Mental Health Issues among IndividualsDocument6 pagesAn Analysis on Mental Health Issues among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget’s Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System for Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System for Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolDocument31 pagesThe Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction using Bi-LSTMDocument8 pagesAir Quality Index Prediction using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict the Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict the Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson’s Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson’s Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation for Translating Global Languages into Indian LanuagesDocument7 pagesHarnessing Open Innovation for Translating Global Languages into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Exploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractDocument7 pagesExploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Electro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyDocument7 pagesElectro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design, Development and Evaluation of Methi-Shikakai Herbal ShampooDocument8 pagesDesign, Development and Evaluation of Methi-Shikakai Herbal ShampooInternational Journal of Innovative Science and Research Technology100% (3)
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Survey of the Plastic Waste used in Paving BlocksDocument4 pagesA Survey of the Plastic Waste used in Paving BlocksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightDocument4 pagesComparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETDocument6 pagesAuto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentDocument7 pagesCyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cardio Oncology Management of Toxicities in The Era of ImmunotherapyDocument127 pagesCardio Oncology Management of Toxicities in The Era of ImmunotherapyRicardo Soto FontalvoNo ratings yet
- CK 7 and CK 20 Positive Tumors Modern Pathol 2000Document11 pagesCK 7 and CK 20 Positive Tumors Modern Pathol 2000api-26176346No ratings yet
- CANCER GRADING VS STAGINGDocument40 pagesCANCER GRADING VS STAGINGKaren Joyce Costales MagtanongNo ratings yet
- Five-Year Outcomes With Pembrolizumab Vs Chemotherapy As First Line in NSCLCDocument7 pagesFive-Year Outcomes With Pembrolizumab Vs Chemotherapy As First Line in NSCLCVu Hong NamNo ratings yet
- Lung Anatomy, Cancers and MesotheliomaDocument60 pagesLung Anatomy, Cancers and MesotheliomaKatNo ratings yet
- 11 Lung CancerDocument30 pages11 Lung CancerMuhammadNo ratings yet
- Management of Lung CancerDocument31 pagesManagement of Lung CancerPadmaj KulkarniNo ratings yet
- bb10 Chap1Document116 pagesbb10 Chap1Dulce Kriselda E. FaigmaniNo ratings yet
- Cisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedDocument2 pagesCisplatin Versus Carboplatin For Patients With Metastatic Non - Small-Cell Lung Cancer - An Old Rivalry RenewedFlorin RizicaNo ratings yet
- Pharma Mar Smart Fund Short ThesisDocument24 pagesPharma Mar Smart Fund Short Thesisjulia skripka-serry20% (5)
- Laboratory and Diagnostic Findings: Small Cell CarcinomaDocument4 pagesLaboratory and Diagnostic Findings: Small Cell CarcinomaTheresa Sombilla FacunlaNo ratings yet
- Internal Medicine Case StudiesDocument56 pagesInternal Medicine Case StudiesLwayNo ratings yet
- Lepechoux 2020Document7 pagesLepechoux 2020Aniketh BaghoriyaNo ratings yet
- Lung Cancer TherapyDocument8 pagesLung Cancer Therapylameck phiriNo ratings yet
- Lung Cancer Thesis PDFDocument4 pagesLung Cancer Thesis PDFykramhiig100% (2)
- Tepotinib in Non-Small-Cell Lung Cancer With MET Exon 14 Skipping Mutations JCDocument4 pagesTepotinib in Non-Small-Cell Lung Cancer With MET Exon 14 Skipping Mutations JCYaramNo ratings yet
- Wiki Resp Mcqs ExplainedDocument7 pagesWiki Resp Mcqs ExplainedArvinth Guna SegaranNo ratings yet
- Makalah Bahasa Inggris NewDocument25 pagesMakalah Bahasa Inggris Newmei diana sara'isNo ratings yet
- 2016 EdBookDocument931 pages2016 EdBookvarun7189100% (1)
- Updates and Management Algorithm For Neuroendocrine Tumors of The Uterine CervixDocument10 pagesUpdates and Management Algorithm For Neuroendocrine Tumors of The Uterine CervixdosiNo ratings yet
- Presentation Small Cell Lung CancerDocument59 pagesPresentation Small Cell Lung Cancerprudhviraj mNo ratings yet
- Icd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test BankDocument11 pagesIcd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test Bankgisellephongejs100% (39)
- 5-Bronchogenic Carcinoma & ParamalignantDocument20 pages5-Bronchogenic Carcinoma & ParamalignantMayar JaradNo ratings yet
- Success Using Soursop Tea and DietDocument4 pagesSuccess Using Soursop Tea and DietKjNo ratings yet
- Мелкоклеточная карциномаDocument250 pagesМелкоклеточная карциномаBertramVrellingNo ratings yet
- Bronchogenic Carcinoma: DR Ayman El-DibDocument40 pagesBronchogenic Carcinoma: DR Ayman El-DibMuhdZaeedNo ratings yet
- Neeman Presentation On OncologyDocument20 pagesNeeman Presentation On Oncologyjlduorah7118100% (1)
- Skeels Handbook of Cancer Therapy 9thnbsped 9781496305558 - CompressDocument954 pagesSkeels Handbook of Cancer Therapy 9thnbsped 9781496305558 - CompressbonitafrancoNo ratings yet
- Lung CancerDocument52 pagesLung CancerHealth Education Library for People50% (4)
- Date 6 Oct 2023Document6 pagesDate 6 Oct 2023mughallaiba901No ratings yet